


Vitamin D
Vitamin D insufficiency and deficiency is a global issue.
 Slides taken from a lecture presentation at the RSM by R A Brown with thanks to the originating authors of the data and related papers.
Slides taken from a lecture presentation at the RSM by R A Brown with thanks to the originating authors of the data and related papers.“The average age of the children was 5.5 years. Three-quarters of them had hypovitaminosis D, and 40% had vitamin D deficiency. Approximately 10% had severe vitamin D deficiency. Children adopted from Ethiopia, Peru, India, Bulgaria, and Lithuania were at significantly higher risk for hypovitaminosis D than others, with more than 90% of these adoptees affected. “

.
 (See below)
(See below)“Chief Medical Officer ‘ashamed’ as rickets makes a comeback“ (Link)
“40 per cent of English children have some kind of vitamin D deficiency ” Independent News Paper story 2013 (Link)
Prevalence and Predictors of Vitamin D Insufficiency in Children: A Great Britain Population Based Study (2011) (Link)
“We confirm a previously under-recognised risk of VDI in adolescents. The marked higher risk for VDI in non-white children suggests they should be targeted in any preventative strategies. The association of higher risk of VDI among children who exercised less outdoors, watched more TV and were overweight highlights potentially modifiable risk factors. Clearer guidelines and an increased awareness especially in adolescents are needed, as there are no recommendations for vitamin D supplementation in older children.”
Vitamin D intake from diet did not affect figures, but supplementation did, as did time spent outside, latitude and household income. The lack of dietary effect may be a mix of fortification of margarines, and other processed foods, low levels in milk and other animal products due to changing farming practices, and limited oily fish intake.
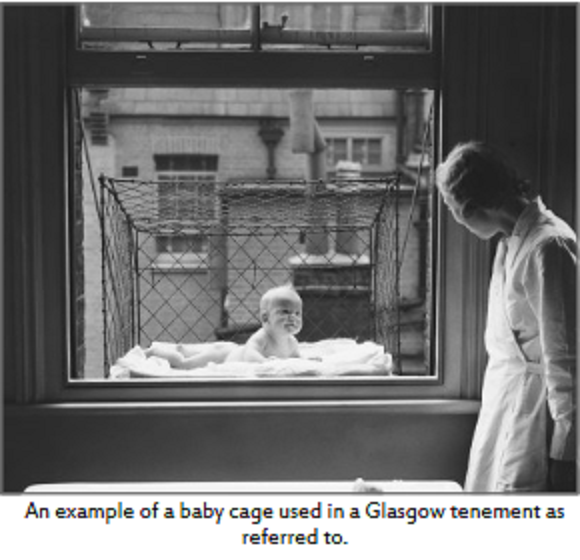
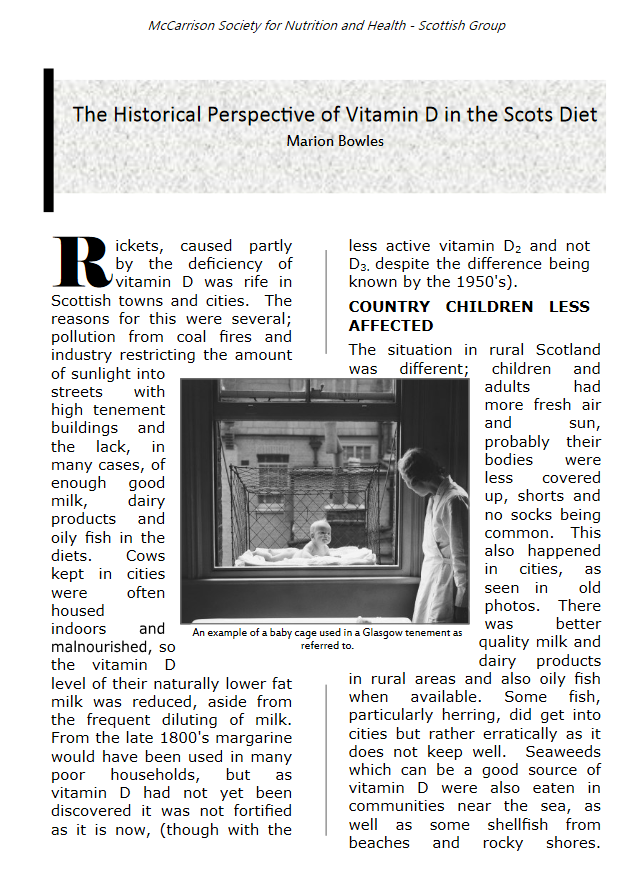
Historic public recognition of the importance of Vitamin D; window cradles in Glasgow tenements, and UV for children in Town Halls; from a Scottish McCarrison Society Newsletter.

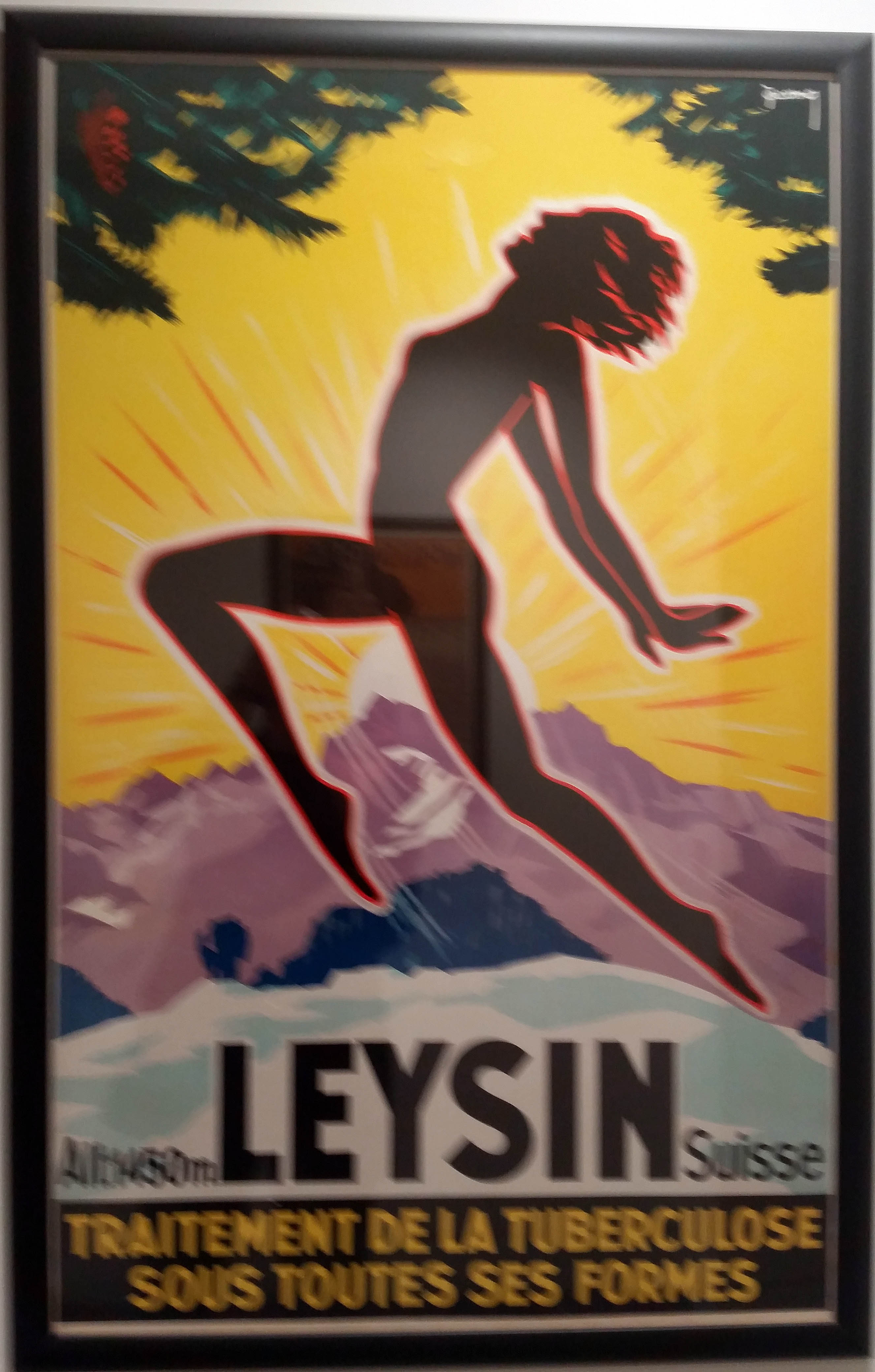
Vitamin D levels are also linked to the risk of incidence of tuberculosis. Heliotherapy, including exposure to sun, was commonly used as a part of tuberculosis treatment. Clinics were set up in the alps, possibly because results were better due to higher UVB penetration at altitude. Modern research suggests that all those patients and Swiss doctors had not lost their capacity to observe and reason; they were right vitamin D appears to reduce infection risk and recovery, as well as improving immune function generally and in specific conditions. (Link)
 Wellcome Trust Library
Wellcome Trust Library
Modern perception of sun exposure and related exposure advice.
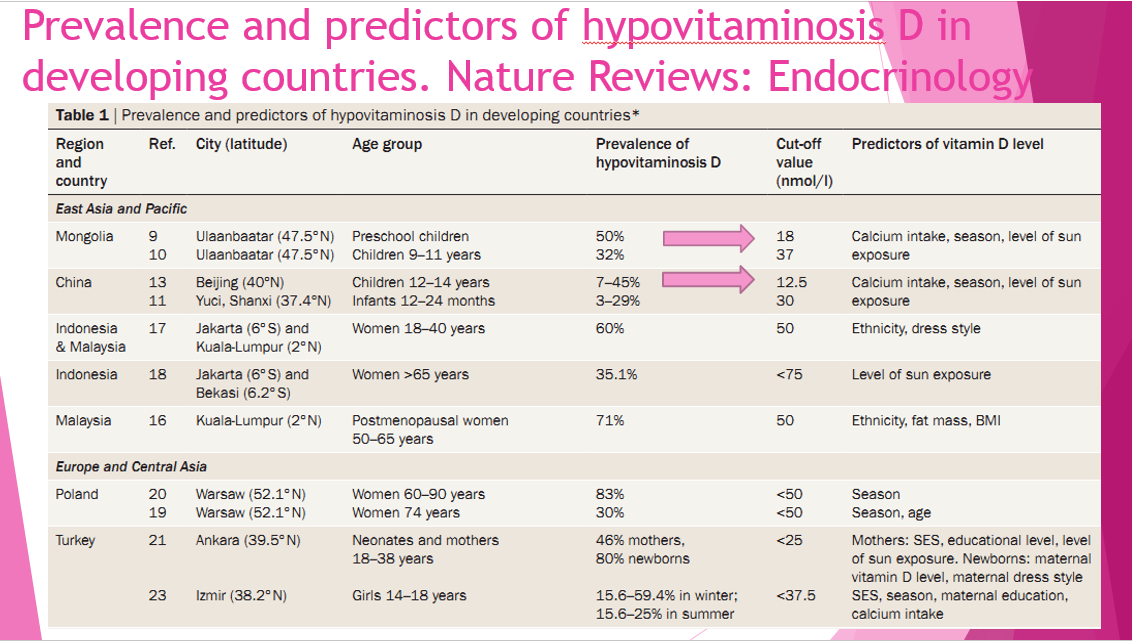
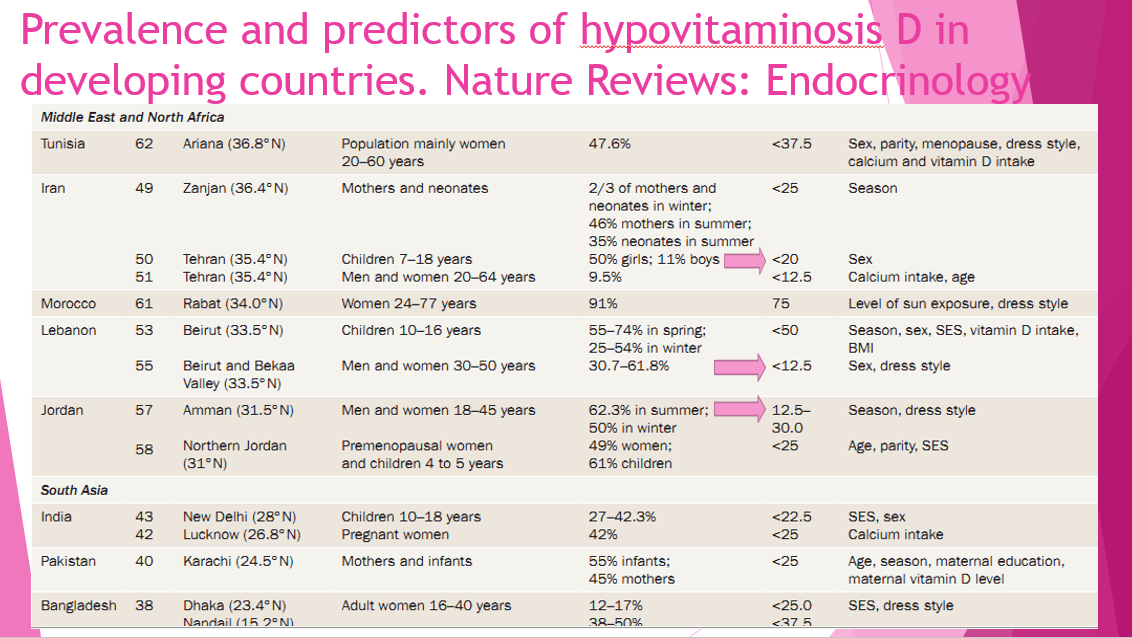
The public perception of the relative benefits and dis-benefits of non-burning exposure to sun has changed, and consequently today significant numbers globally are insufficient or deficient in Vitamin D. (See tables above)
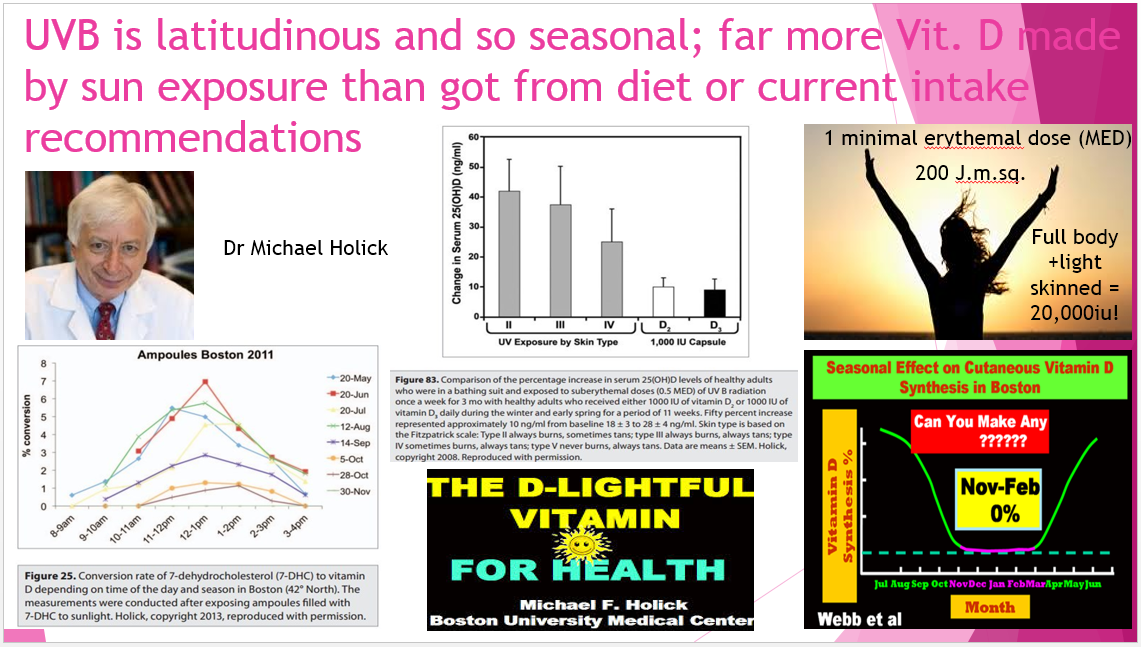
Several studies suggest sun exposure is by far the largest source of Vitamin D in humans, and Michael Holick (Video below or here (Link)) suggests up to 90% of human Vitamin D is derived from sun exposure.
 Slide taken from a lecture presentation at the RSM by R A Brown with thanks to the originating authors of the data and related papers.
Slide taken from a lecture presentation at the RSM by R A Brown with thanks to the originating authors of the data and related papers.
Somebody with a fair skin exposed to the point of very slight pinkness who has not seen the sun for a while can make 20,000IU of vitamin D, which would require drinking 2000 glasses of milk or more, (depending if the cows got outside and or got grass to eat), and even a lot of Cornflakes (see below).
Typical sun advice
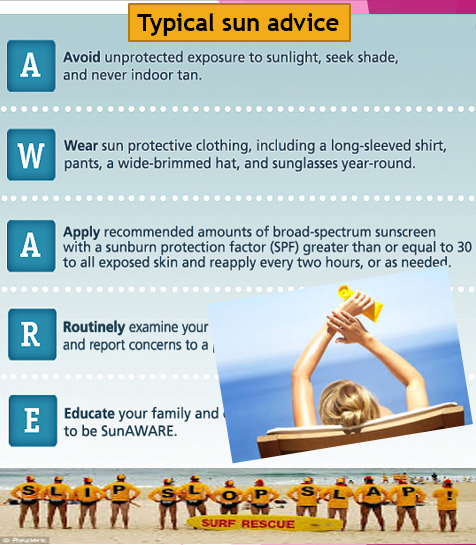
This is the current typical sun advice message, based on looking at the risk of melanoma, but without considering or advising on wider implications of vitamin D insufficiency of deficiency, such as reduction of immune function, including for example greater susceptibility to tuberculosis. (Link)(Link)
The message is to stay out of the sun unless sunblock is applied is widespread arguably so prevalent because it facilities the sale of sun blockers, and so there are commercially available funds to support education and promulgation, which then becomes self- propelling.
For those concerned about facial ageing ( are not we all 🙂 ) the face apparently makes limited vitamin D, so the extensive use of UV blocker will have less impact there than the ‘permanent’ use of blockers on arms and legs etc.
In contrast, preventing for example less visible tuberculosis spread, including through vitamin D production by approriate non-burning sun exposure, does not have the same commercial impetus.
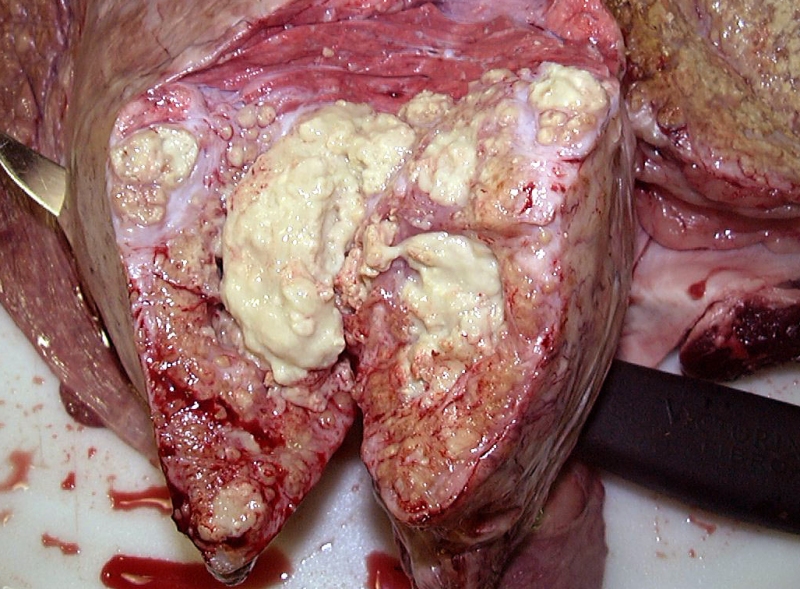 Bovine tuberculosis (Link)
Bovine tuberculosis (Link)
Neither does prevention of tooth decay by means other than proprietory dental cleansing products.
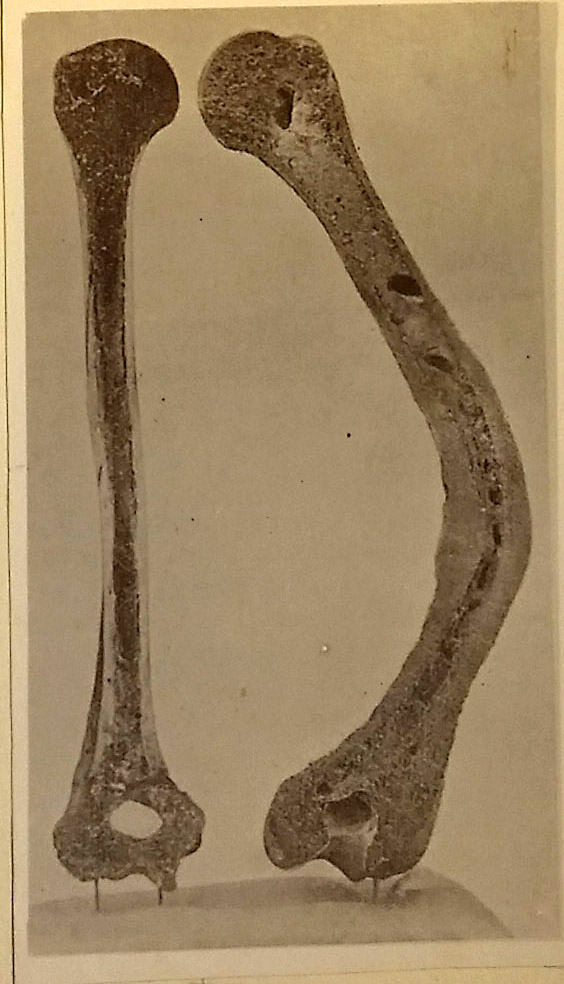
As well as bone formation and immune function, Vitamin D influences a host of other pathways as can be see from the huge variety of papers collected on VitaminDWiki (Link). Thought-provokingly it is essential to brain formation in utero, and impacts pelvic arch formation; low vitamin D may result in reduced pelvic arch width (Link) so birthing.
The obese tend to have lower blood levels of vitamin D as it is sequestered into fat tissue. Vitamin D is a factor in obesity as it effects mitochondrial metabolism. It also affects gut integrity as it impacts cell junction function so is likely a significant factor in gut disorders, and related inflammatory conditions. It has potential roles in antioxidant pathways. It is also a potential factor in diabetes type 1 and possibly in autism.
Weighing the relative risks, individual and societal consequences of the impact lower UV from exposure to sunshine on melanoma v the effects of consequent vitamin D insufficiencies, including on increased incidence and progression of other diseases including dental decay and tuberculosis (Link) is not for the McCarrison Society, but clearly there should be wider education including of doctors as to the importance of vitamin D. In contrast to the UK in Europe ensuring adequate vitamin D, particularly for pregnant women and infants, is mandated as a high priority issue for doctors.
How much vitamin D is in food, and how much do we need?

Slides taken from a lecture presentation at the RSM by R A Brown with thanks to the originating authors of the data and related papers.
The amount of vitamin D in foods compared to the amount that can be made in the skin (20,000 IU in the light skinned) is small. Few foods contain significant vitamin D including, oily fish (farmed less than wild) and sun exposed mushrooms. Cattle, pigs and hens make vitamin D from sun-exposure, and get some from feed particularly aged sun exposed pastures; they now live indoors and often do not get to see much grass, which feeds through to lower vitamin D in eggs, milk and carcass fat.
Low levels of supplementation 400iu a day in those who are not deficient, may be of benefit, but will not make a huge difference to blood levels. The topic of how vitamin D supplement intake impacts on blood levels is looked at in this paper (Link) from Grass Roots Health (Link) a campaigning organisation who commissioned this research to try and answer the question what are optimal vitamin D levels, among others.
This video below is of Carole Baggerly who set up Grass Roots Health, a wonderful insight into the background and ethics of Carol and the organisation, and provides powerful research data as to the reduction in the risk of a range of diseases, including breast cancer occurrence and re-occurrence, and diabetes type 1, with increased vitamin D levels, as well as providing information as to intake levels and safety.
What about those with dark skins do they make and need vitamin D
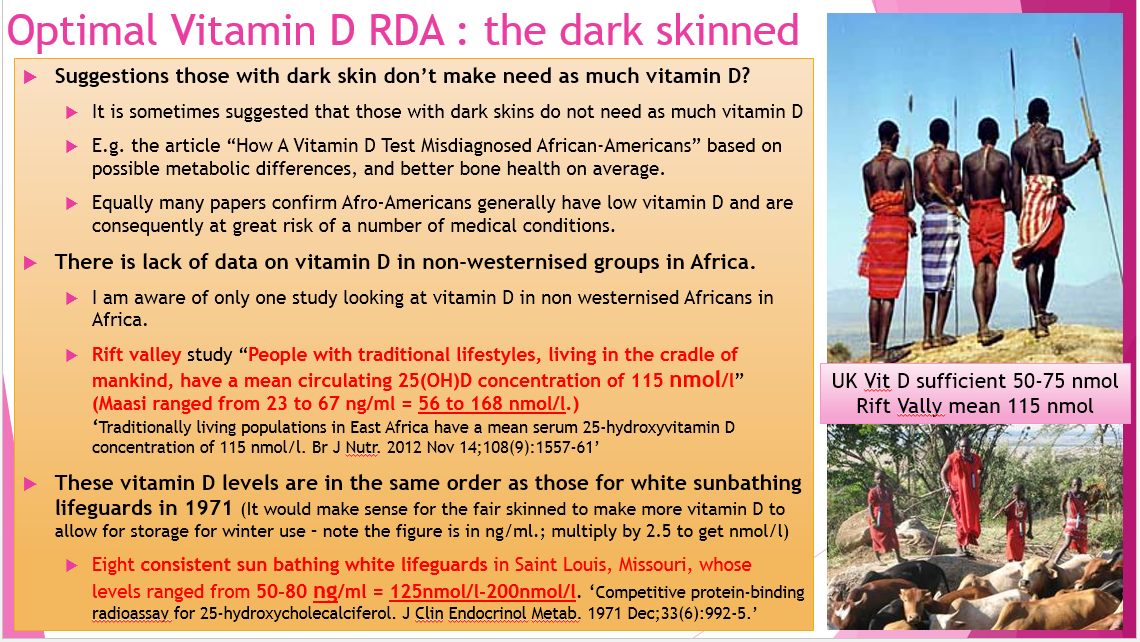 Those with dark skins have powerful built in sunscreens that vary with skin tone. They can and do make high levels of vitamin D, but need more sun exposure time to do so. Sadly there has been very little research in this area, hence one of our aspirational projects is too promote further studies on vitamin D levels in non-westernised groups, whilst some still remain (Link).
Those with dark skins have powerful built in sunscreens that vary with skin tone. They can and do make high levels of vitamin D, but need more sun exposure time to do so. Sadly there has been very little research in this area, hence one of our aspirational projects is too promote further studies on vitamin D levels in non-westernised groups, whilst some still remain (Link).
Vitamin D levels in dark skinned people in northern latitudes tend to be lower than those in light skinned, and low Vitamin D is a global issue. Levels in pregnant women with dark skins are often frighteningly low.
Risks of vitamin D deficiency in pregnancy and infancy.
This paper Nutritional Rickets by Behzat Özkan J Clin Res Pediatr Endocrinol. 2010 Dec; 2(4): 137–143. available here (Link) very helpfully sets out important back ground material including the following thought provoking excerpts. The content of the paper makes clear the effects of vitamin D deficiency on health are significant.
Scope of incidence
“Nutritional rickets (NR) is still the most common form of growing bone disease despite the efforts of health care providers to reduce the incidence of the disease.”
“In 2005, the Turkish Ministry of Health initiated a campaign of free vitamin D for every infant”
Risk Factors
” Limited sunshine exposure due to individuals’ spending more time indoors (watching television and working on computer) or avoiding sun exposure intentionally for fear of skin cancer. Traditional clothing (covering the entire body except the face and hands) further limits the exposure time to sunlight “
Risk factors are helpfully tabulated here (Link)
Health Consequences
“In addition to its short− or long−term effects on skeletal development, VDD during infancy may predispose the patient to diseases such as diabetes mellitus, cancer and multiple sclerosis. “
“findings specific to the bone tissue in rickets include craniotabes in infants older than 2−3 months, delayed fontanel closure, enlargement of wrists, rachitic rosary, delayed teething, carious teeth, enamel hypoplasia, “O“− or “X“−type leg deformity, kyphosis and a narrow pelvis that may affect labor in later years, chest deformities such as Harrison’s groove and pigeon breast, costal or lower extremity fractures (particularly greenstick fractures),”
“Physical examination findings not specific to the bone tissue include hypocalcemic convulsions, hypotonia, constipation, proximal myopathy, heart failure, anemia, pancytopenia, cardiomyopathy, benign intracranial hypertension, growth retardation and low height−for−age”
Prevention recommendations in sunny Turkey
The Bone Health Group in Turkey recommends vitamin D supplementation of at least 400 IU/day to be introduced at birth and continued until sufficient vitamin D is provided by the diet. However, it is argued that this dose will prevent the development of clinical rickets, but will fail to prevent vitamin D insufficiency. Therefore, different doses of vitamin D, depending on the risk level, need to be administered for the prophylaxis of VDD. Accordingly, the dose of prophylactic vitamin D is 800 IU/day during winter months in Canada, whereas the dose is 400 IU/day in summer. The dose is 800 IU/day all year round in Bulgaria and 400 IU/day all year round in Romania (29, 33, 34, 35, 36). The Turkish Ministry of Health encourages vitamin D to be administered at a minimum dose of 400 IU/day until 1 year of age for all infants starting from birth, regardless of type of nutrition (9).
Conclusion of Turkish Paper
“In conclusion, the vitamin D requirement of a growing child has not clearly been identified. However, we know that children need more vitamin D than the current amounts provided (36). It is up to mothers to supply their children with more Ca−rich foods and sunlight in order to ensure that the vitamin D and Ca requirement of both themselves and their infants is met by natural means.”
Further if a mothers vitamin D status is low her breast milk is unlikely to contain sufficient vitamin D, putting her infant at risk of vitamin D deficiency or insufficiency. A paper titled Vitamin D and calcium in the human breast milk states “The adequate intake of vitamin D in infants up to 12 months is 400 IU (10mg) with sensible sun exposure. Infants require up to 30 min of sunlight per week wearing only a diaper and 2 h per week fully clothed with no hat. The daily requirement recommended by the Endocrine Practice Guide-lines Committee for this age group is 400-1000 IU with the tolerable upper intake level of 2000 IU. The current recommendations of the Americans Academy of Pediatrics is that all breastfed infants be supplemented with 400 IU/d of oral vitamin D from birth.” (Link)
(See also Holick video above) Dr Holick offers similar advice. Care should be taken with supplementation as overdosing of babies in error is not unknown. (LInk)
Recommendations vary between countries. Mother should seek advice from their doctors. The above does not constitute medical advice, it is simply intended to act as generalised education material.
Vitamin D intake importance to bone and tooth structure, formation, carie resistance and remineralisation
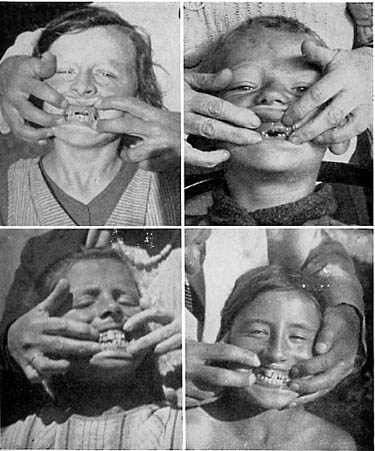
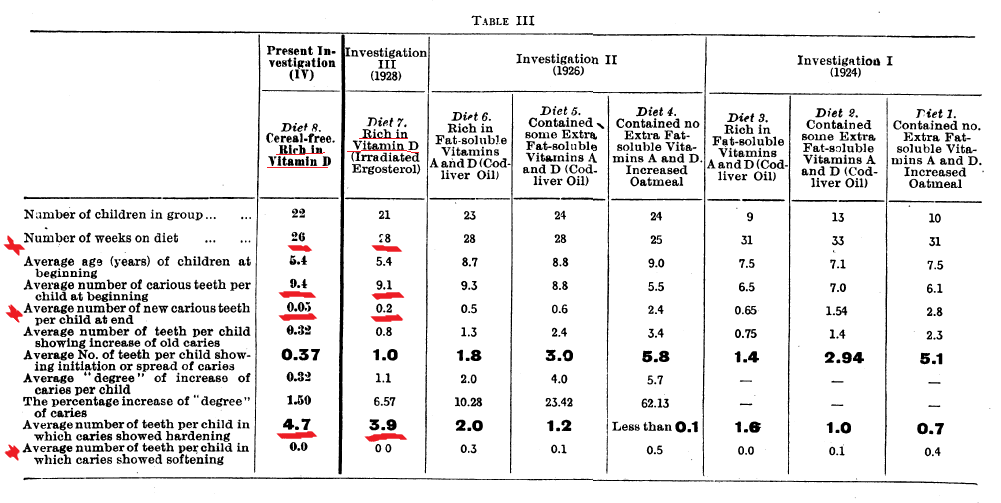
The Mellanby’s (Link) did research on vitamin D and dental formation which was truly seminal, yet it appears in part forgotten. Their work showed that vitamin D as well as being essential for the prevention of rickets, was central to the formation, and interior bone structure of teeth, and related to reduction in caries and improved remineralisation. A BMJ paper in 1932 by May Mellanby, one of many on the topic of vitamin D by the Mellanbys, available below states:
“It has been shown that normal, well-developed teeth are more resistant to caries than poorly developed (hvpoplastic) teeth. Since the majority of human teeth in this country are defective in structure, it would seem that one method of reducing the incidence of dental caries should be the production of teeth of good structure by suitable diets, both for mothers during pregnancy and lactation, and for their offspring during the period of tooth calcification. This is essentially the prophylactic method of attacking dental canes.”
Adequate vitamin D was essential for resistance to decay and re-mineralisation (See table below). The effect was reduced by phytates in grains. We are not told the dosage of vitamin D so do not know if higher levels of vitamin d would counteract the effects of phytates in grain. The health of Hunza and Sikhs as reported by McCarrison would suggest that the effect or fresh grains is not an overriding factor in dental health, but both had access to calcium rich dairy products. Weston Price reported oats were a staple of Scottish Islanders, and noted they had outstanding teeth. (Ch. 4 Isolated and modernized Gaelics Link) Many cultures traditionally often fermentation or cooked grains for long time frames (eg traditional porridge slow cooked overnight) which may reduce phytates.
Given that in 2016 vitamin D insufficiency and deficiency is widespread in mothers and infants, it would be logical to expect to see emergence of increased dental decay and poorer tooth formation despite, both dental hygiene products, and application of fluoride which hardens the enamel surface, but does not impact inner structures in the same way. Press and anecdotal reports reports suggest dental decay and related hospital extractions are indeed still rising.
A dentist suggested anecdotally that enamels were harder, but once penetration of enamel occurred decay was happening at very rapid rates compared to years ago, suggesting poorer quality formation of internal tooth structures.
Risks of increase melanomas due to sun exposure in infancy.
One of the reasons in addition to changing lifestyles for reductions in exposure to sun so vitamin D in people of all ages is a combination of health sun awareness messages and understandable fear of skin cancer. There is some evidence that excess sun exposure at all ages is a factor in increased occurrence of melanomas.
However the reasons for increasing melanoma incidence, whilst potentially significantly triggered by excess UV exposure are likely multifactoral, including dietary changes, lifestyle changes including more time behind glass in the sun, and potentially use of some skin products, but rarely considered as such, which is partly the consequence of specialisation and lack of integration of different research fields, as well as the existence of commercial markets for sunscreens, but limited commercial prospects for research outcomes, for example in examination of lipid imbalances and iodine insufficiencies in relation to skin responses to UVA and UVB .
The 1994 paper Melanoma: prevention and early diagnosis Joan Austoker published in the BMJ provides very useful background information, including
“Skin cancer: current facts
Skin cancers are common in many parts of the world, and the number of cases is increasing. In the United Kingdom there are some 40000 new cases each year. There are three main types of skin cancer. The most frequently occurring types are basal cell carcinoma (rodent ulcer) and squamous cell carcinoma, both of which tend to occur in older people. Over 95% of these types of skin cancer are curable. They can, how-ever, be disfiguring if not diagnosed and treated early.“
The third type is malignant melanoma, which is comparatively rare (11% of all skin cancers). There are four main types of melanoma (table I). There were 4438 new cases of melanoma in the United Kingdom in 1988, but this is probably an underestimation because of incomplete ascertainment (except in Scotland).
There are roughly six to seven cases in women for every four cases in men.
Wider useful information is set out in a Technical Report – Ultraviolet Radiation: A Harzard to Children and Adolescents. (Link) a paper by the American Academy of Pediatrics. Whilst this paper considers vitamin D, in common with many papers on the subject is UV-centric.
Commercial drivers exist for focus on UV as a cause of melanoma, although there are likely to be multifactoral contributory factors including diet.
As discussed the market and commercial opportunities for UV blocking skin products are significant, which in turn provides funding for educational messages, research, employment so together creating a UV-centric outlook on skin damage including skin cancers.
In consequences other factors that may influence the way the skin ages and reacts to UV such as; vitamin D levels, iodine levels, omega 3 and 6 polyunsaturated fat intake, and other dietary factors such as minerals and lipid soluble antioxidants, including from dietary plant intakes, whilst likely factoring in changing rates of skin cancer, comparatively receive relatively little attention.
Iodine is important to skin function, as are polyunsaturated lipids, and both have roles in redox pathways. There are indications. but limited research, suggesting that iodine levels, and Omega 3 intake increase / and or reduction in Omega 6 intake, extend non-burning sun exposure time and reduce the incidence of burning.
Anecdotal reports suggest iodine may moderate the risk of melanoma, or topical application may reduce it once it has occurred, but little if any research has been done into the area. Iodine intake and Omega 3 would have been higher in shoreline peoples including potentially fair-skinned ‘Celts’ who in evolutionary timescales may have had greater UV exposure.
Further the early ‘sun cream’ product focused on UVB blockers to the exclusion of UVA, and promotion of them as allowing greater non-burning exposure to sun, may unwittingly have contributed through reduced vitamin D levels and increased UVA exposure to increased risks of DNA and other damage, which may have been a contributory factors in cancers, although study outcomes conflict. This may in turn have been one of several synergistic factors, including dietary changes, leading to the rise in skin cancer rates, .
There is now recognition UVA may be a factor in skin cancer, and many sun products now seek to protect against UVA and UVB.
Blocking UVB action also blocks the ability of the body to make vitamin D and related downstream oxidised derivatives, which are part of the skins sun protection mechanisms. It is the UVB oxidised lipid and related products, which trigger the pain and inflammation related signalling that tells us the skin’s antioxidiant capacity is becoming exhausted, and we need to seek shade.
Blocking of this signalling may UVB blockers arguably allows extended exposure so potentially damage to deeper skin layers by UVA.
Relevance to tuberculosis of diet and other factors including UVB exposure – research by McCarrison Mellanby etc.
McCarrison, Mellanby, Weston Price, Pottenger, Sinclair and others; all in effect early researchers in deficiency diseases, from different positions all essentially took position later distilled by Sinclair (Link) into a simple but fundamental self evident but often forgotten unavoidable reality, and consequent on our biology, that nutrients including minerals were essential to cellular function so health:
“The deficiency of any nutrient which is essential for every tissue will eventually lead to abnormal function in every tissue. That is so incontrovertibly obvious that I am continually astonished by the eminence of the medical scientists to whom it must be forcefully restated.”
“The second is that when deprivation of an essential nutrient occurs, not all tissues will be simultaneously and equally affected, and not all individuals will react in the same way. Which tissue shows symptoms first will depend on the genetic inheritance of the individual and on his or her exposure to environmental factors and lifestyle events.”
They realised that pathways were interlinked and synergistic, and that absence or excess of a particular nutrient may impact on the requirement for another.
They noted that well fed study animals were more resistant to a range of conditions and that one or more individual nutrient deficiencies could be associated with the onset and progression of particular conditions.
In the commercial driven race to understand biological pathways often for the purposes of creating commercial products we have arguably lost sight of the ability of diet to moderate disease, and more particularly of the insufficiency or deficiency or particular nutrients such as vitamin D and iodine to exacerbate even lead to the onset of a wide range of debilitating, as well as ‘expensive’ medical and health related conditions.
Paraphrasing the words of Dr Burkitt in the admirable quest to improve our capacity technology and expertise in mopping floors, we should not forget we need also to turn of the taps of disease.
“Don’t Just Mop the Floor; Turn the Taps Off”
Dr D Burkitt (Link)
.
Vitamin D wiki a wondrous resource and testament to ones mans foresight and determination.
An excellent site set up by an individual, a retired electronic engineer, who came to realise the importance of vitamin D.
A few of the links posted on HER2 Support
http://jcem.endojournals.org/cgi/con…ract/90/6/3215
http://grande.nal.usda.gov/ibids/ind…&therow=110910
5 must watch videos