


(This page will be added to over time)
A dental paradigm
The segmentation of education with little attention on prevention, means the medical and dental profession get little training in the relevance of wider nutrition, beyond reducing sugar intake.
Despite low vitamin D being a widespread global issue, and other nutritional insufficiencies increasingly commonplace, dentists will talk to patients about argued benefits of flouride, and danger of sugar and sweets, but will as a generality rarely raise the question of vitamin D or wider fat soluble vitamin status, or advise on wider diet.
Work in the 1920s and 30s demonstrated fat soluble vitamin D, A, and K2 then suggested by Weston Price to be factor X, are essential to tooth formation during pregnancy, in early childhood, and important to decay risk reduction throughout the life course.
Fat soluble vitamin K2 is likely central to bone metabolism including through the osteocalcin pathway, so logically also dental health, although research into vitamin K2 and dental health is limited.
Limited but detailed studies in the 1920s, including work by Mrs Mellanby (see below), suggest vitamin A is important to dental including enamel formation during pregnancy. Effects of deficiency during formation include “atrophy and metaplasia of the enamel organ and atrophy of odnotoblasts, accompanied by atypical formation of dentine” (Link) However excess vitamin A can inhibit bone repair, so logically excess may also negatively impact dental health. (Link)
Other dietary factors, including likely iodine, and wider mineral sufficiency, are also essential to bone growth, as well as likely control of oral bacteria. When iodine is administered a significant amount is directed to the oral area including salivary glands. Those with iodine deficiencies generally exhibit lower than average growth, and may show signs of sub-optimal skeletal formation, as well as impaired dental formation. (Link) “iodine deficiency in the diet of animals entailed abnormalities in the growth patterns, destructive alterations in the bones and bone marrow, a decrease in the content of hydroxyproline, hexosamines, and in the activity of phosphomonoesterase-I in animal bones, as well as disorders of phosphocalcium metabolism” (Link)
Rates of dental decay in the young in the UK are significant.
“Nearly half of eight-year-olds and a third of five-year-olds have signs of decay in their milk teeth, a national dental health survey has found.” BBC 2015 (Link)
“The Faculty of Dental Surgery at the Royal College of Surgeons of England is seriously concerned about the state of children’s oral health in England. Almost a third of five-year-olds are suffering from tooth decay, there are significant regional inequalities, and it is the most common single reason why five- to nine-year-olds are admitted to hospital. In some cases children are admitted for multiple tooth extractions under general anaesthetic, despite tooth decay being almost entirely preventable.” The state of children’s oral health in England. FDS (RCS) report 2015 (Link)
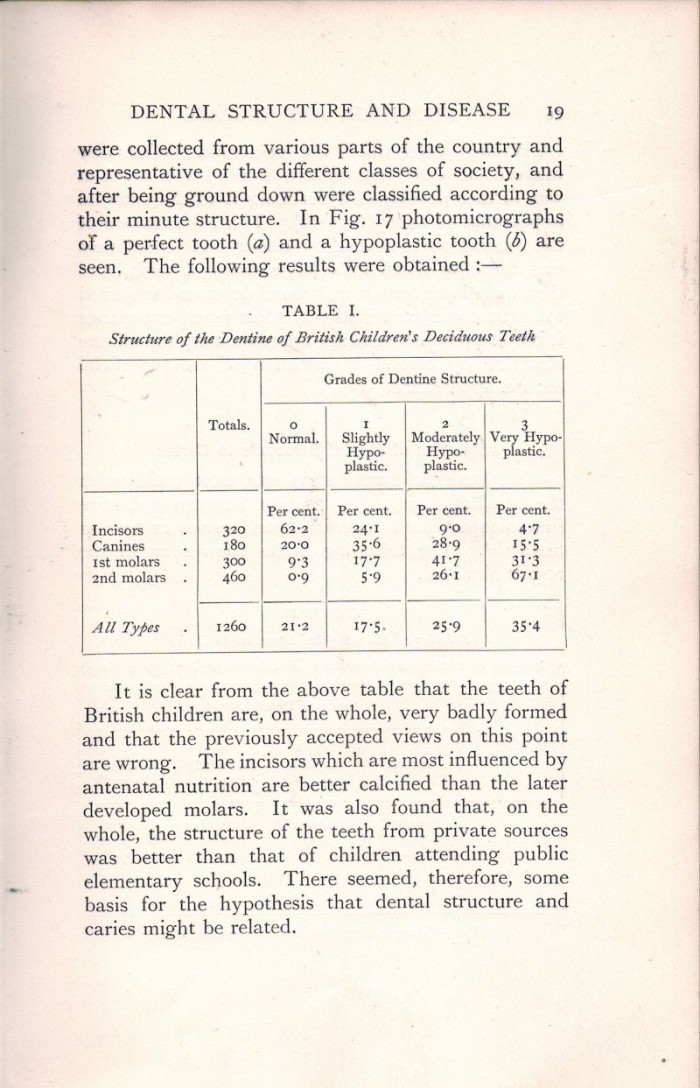 .
.Arguably the work by Mrs Mellanby (Ch 2 ‘Dental Structure and Disease’ by May Mellanby) (Link), which chimes loudly with that of Weston Price (Link), is compulsory reading for anybody who is interested in the topic and idea that diet generally, and particularly some key dietary factors could greatly reduce, even eliminate tooth decay, as well as leading to remineralisation of decayed teeth.
The fat soluble vitamins A and D found in fish oil were found to be particularly relevant to dental and gum health. (see also Vitamin D page (Link))
Fish oil as then extracted likely contained significant vitamin A, D, and some iodine as well as Omega 3 fatty acids, insufficiency of any of which negatively impact wider oral health including risk of periodontal disease.
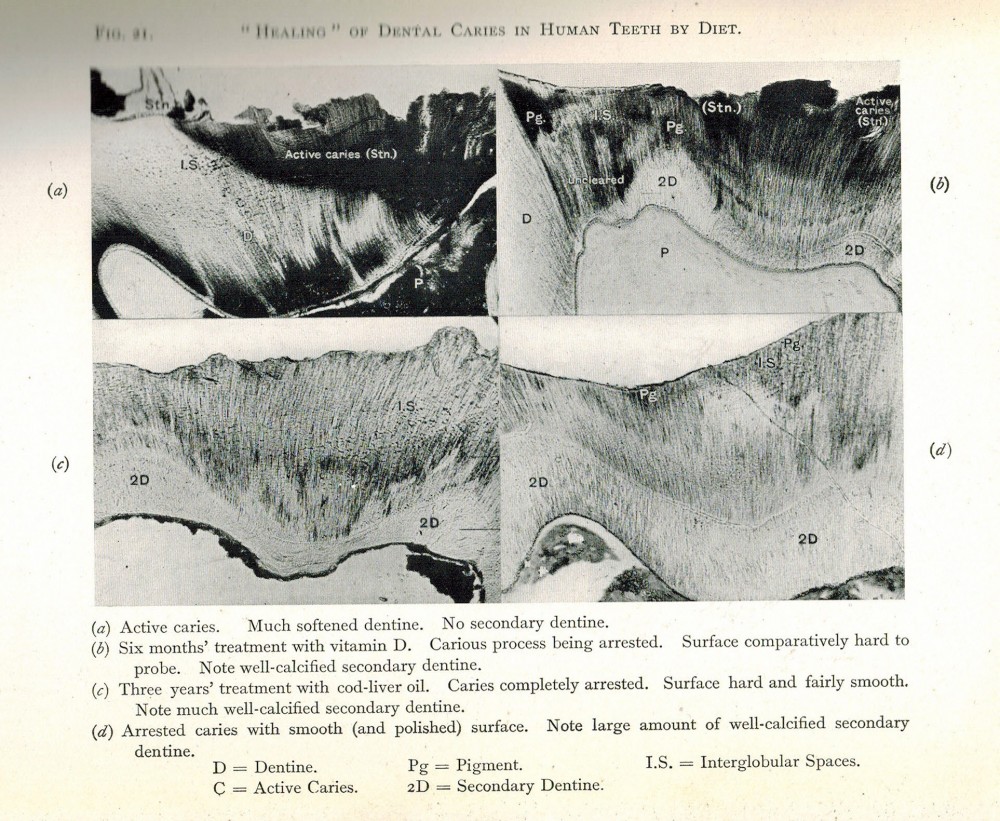
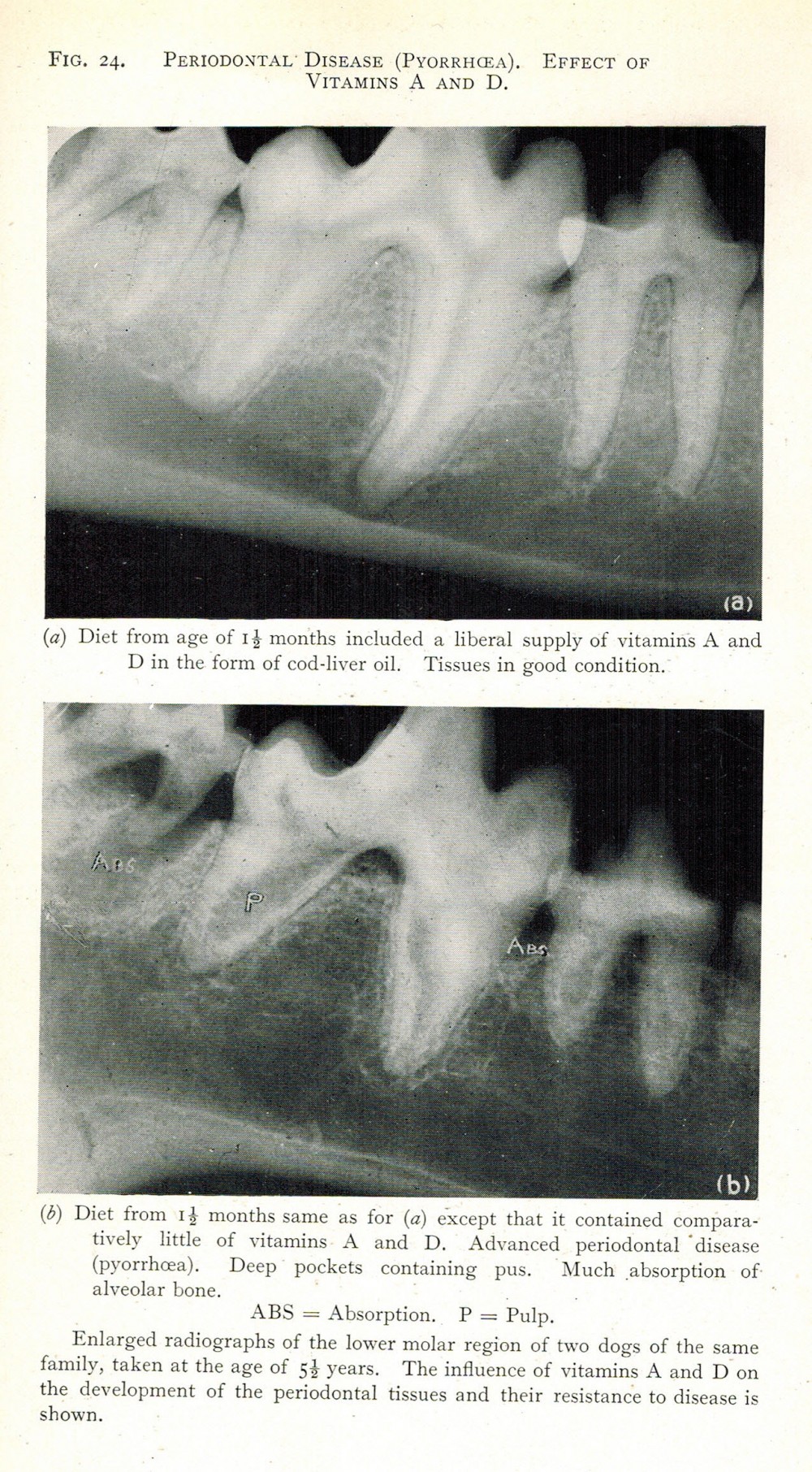
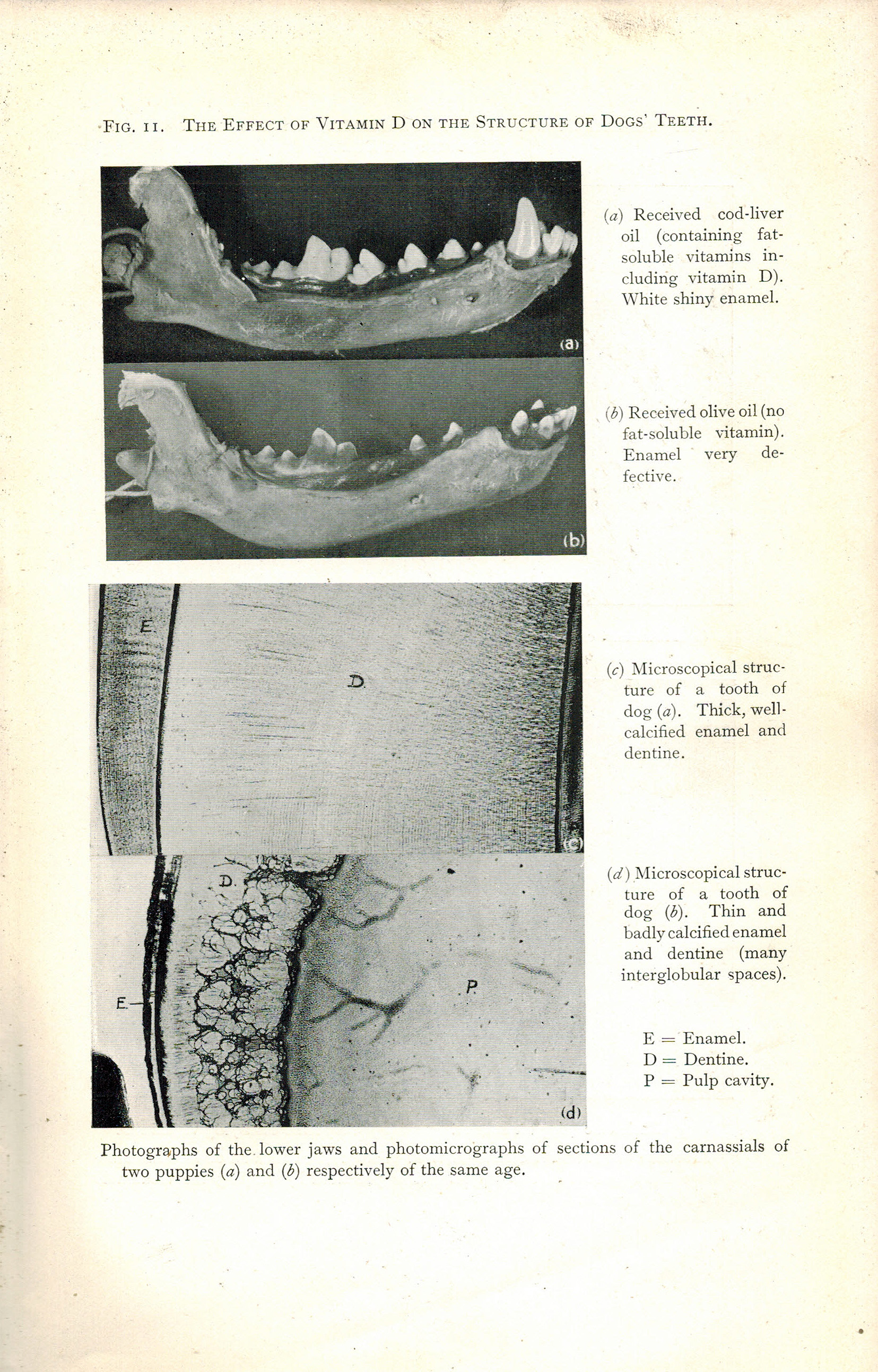
These thought provoking slides are taken from Ch 2 ‘Dental Structure and Disease’ by May Mellanby in the Mellanby’s 1934 book ‘Nutrition and Disease’ available in full (many more powerful informative dental x-ray slides) here (Link).
The first shows repair of dental caries, the second reduction in periodontal disease including deep pus pockets, the third the differences in dental formation in dogs sufficient and insufficient in fat soluble vitamins likely A and D.
 .
.
Halting of decay and tooth remineralisation through diet – authoritative 1930s British Medical Journal (BMJ) paper by leading then researchers
This Mellanby 1930s table shows the reduction in decay and remineralisation of decayed teeth they were able to achieve simply by changes to diet and addition of vitamin D ( The PDF of the full paper can be found here (Link).) Adequate supply of calcium was also found to be a key factor; in the absence of adequate calcium Vitamin D was not effective. Calcium also binds with so mitigates the effect of phytates in grain products.
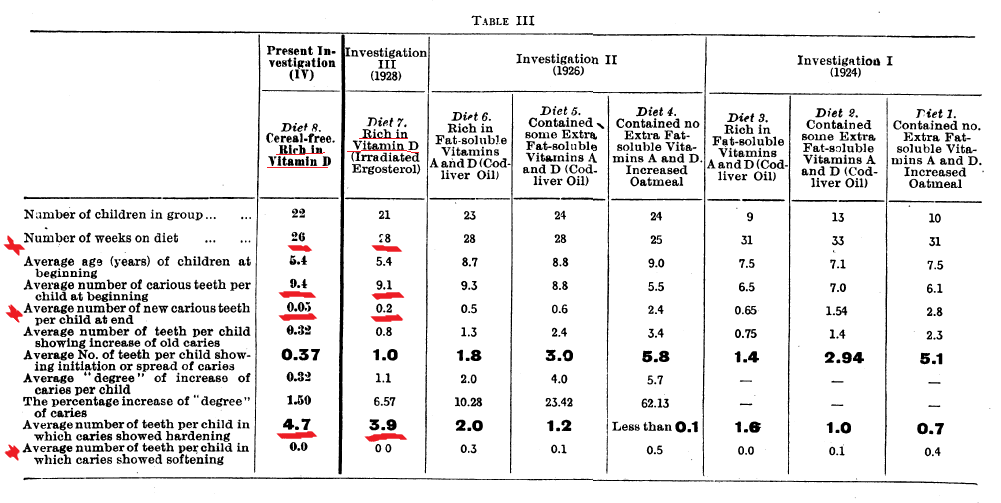 The finding in the above and related papers resulted in the then Government introducing free school milk and cod liver oil, to try and combat ill-health, including tooth decay, due to nutritional deficiency.
The finding in the above and related papers resulted in the then Government introducing free school milk and cod liver oil, to try and combat ill-health, including tooth decay, due to nutritional deficiency.
Significant improvement in children’s dental health 1929-1947
High extraction flour (minimal removal of bran) was made mandatory in WWII, and calcium was added to all loaves to balance out the greater phytates in flour due to increased bran content.
Mellanby (below) emphasises the interrelationship between vitamins A, D and calcium in the formation of health teeth and bones. The inclusion of full fat milk, butter and eggs in the diet, was seen as fundamental because they provided the vitamin A, D and calcium necessary to compliment the other nutrients including in high extraction wat-time flour, in the creation of good bones and skeletal structures. Interestingly dairy was a feature of the Sikh diet.
In WWII, several measures of health improved, including neonatal outcomes, female diabetes mortality reduced (male rates were not recorded with sufficient accuracy due to the war), and decay rates in children decreased significantly.
There was some, but not huge reduction in sugar intake, and interestingly in fat intake.
The observations of Mellanby on improved dental health in WWII in children, in his chapter on ‘Cereals and Calcification’ in ‘Nutritional Research’ published in 1950, are digitised in part below:
It is all about sugar; isn’t it ? ? ?
The current focus, including it appears of guilt ridden parents, is very much on sugar, which narrow focus is arguably detracting attention from wider historic hard won knowledge on the importance of vitamin D, other fat soluble vitamins, and minerals including calcium, on tooth formation, decay and remineralisation.
“If your child has tooth decay, you must be a terrible parent – like me“
Daily Telegraph article banner 15th April 2016 (Link)
Were parents, dentists, doctors and wider heath providers given this information, extents of tooth decay in children would be reduced, and parents would at least not be burdened with as much ‘tooth guilt’
Refined sugar is unquestionably a risk factor for tooth decay, but things are rarely simple. In contrast to refined sugar intake, the role of sugar containing natural foods and their on impact tooth decay rates, is complex. For example cane sugar workers, who generally eat a lot of raw cane sugar, do not have significant increases in decay and some have reduction. (Link) Whole foods contain a complex basket of bio-active products which may moderate the effects of the sugar they contain though both mineral movement / availability, and because they contain plant biocides against bacteria (plant pigments etc.).
Vitamin D is central to bone and tooth formation
As can be seen in the Mellanby BMJ table above, vitamin D levels are key to bone formation. Very few people had well formed second molars, begging a heap of questions about what it takes to get perfectly formed molars, and who round the world has them.
Tooth formation starts in utero. Well formed teeth in utereo are more decay resistant irrespective of later diet. (see Mellanby chapter above p.17). Women who are early term tend to have more decay, which could be a consequence of nutrient demand by the growing baby in utero, and synergistically low nutrients in the mother make it more difficult for the baby in utero to get the nutrients it needs for optimal bone and tooth formation.
As discussed in the vitamin D page, deficiency in the UK and globally is serious and very widespread, including in pregnancy (Link). It is logically likely that women, who compared to males intrinsically have fairer skin and a greater capacity to make and need for vitamin D, particularly in pregnancy, will have lower vitamin D levels due to the extensive presence of UV blockers in skin products, and pervasive messages to stay out of the sun to avoid skin damage. Those with darker skins are at greatest risk.
. Slides taken from a lecture presentation at the RSM by R A Brown with thanks to the originating authors of the data and related papers.
Slides taken from a lecture presentation at the RSM by R A Brown with thanks to the originating authors of the data and related papers.
In the above Mellanby paper, whilst the amount of additional vitamin D is not shown, and the results relate to foods in the 1930s which would have contained, more vitamin D (because livestock were out doors), higher minerals, plant antioxidants etc). The ‘tooth repairing’ ‘diet 8’, apart from the exclusion of grain, is a fairly ordinary diet, and included desserts which would have contained limited sugar. (Weston Price (Link) achieved remineralisation with a diet that included whole gain fresh ground flour rolls – the issue with grains may be processing including fine grinding, bleaching, nutrient removal/oxidation etc, rather than the grains themselves – more research required – interestingly groups on non-westen diets, even those including grains, generally had low rates of decay until they moved to western refined diets. Also rather than vegetable fats, they used minimally processed animal fats, which would have been richer in A, D, iodine etc. Fried and oil roasted meats would have been rare or at least uncommon. Stewed and steamed meats were more prevalent.)
Mineral intakes have likely fallen, based on the fall in content in a basket of minerals in foods over the last 50 years (Link). Bone stock would have probably been used, and is a useful source of nutrients. (Link)(see pages 508 509)
The above suggests in considering dental and wider health that it is important to focus on all aspects of ‘diet’, food preparation and lifestyle, from farm to fork, and not just single components.
Lack of dietary education and or focus of the Dental Profession?
Consequent on a childhood hockey accident, root fillings, consequent infections including in bone, I have sadly sat in quite a number of dentists chairs over many years. With the greatest respect admiration and appreciation, for the skills and dedication of dentists, none have ever mentioned, vitamin A, D, Iodine, minerals or Omega 3s in relation to decay or dental health.
I am immensely grateful to dentists for some excellent restorative work, but deeply saddened that this almost century old information on dental formation, health and decay from the 1920s and 30’s has not been retained, and expanded with additional research.
Teeth are arguably a window to wider health including nutritional status. In addition dental infections can and arguably do lead to wider systemic health issues as identified by Weston Price in the 1920. (Link)
Wider systemic impacts of bacteria of oral origin
Today in 2016 there is growing acceptance, as postulated by Price and others in the 1920s, that bacterial infections of oral origin may have roles in some cardiac related conditions. “There are over 1,000 case reports associating dental procedures or disease with the onset of endocarditis (32).”
At the time the idea did not receive much support, but modern technology and ability to identify and track unique oral bacteria has confirmed oral bacteria can be a source of wider body infections. A paper “Systemic Diseases Caused by Oral Infection” (Link) states:
“Recent progress in classification and identification of oral microorganisms and the realization that certain microorganisms are normally found only in the oral cavity have opened the way for a more realistic assessment of the importance of oral focal infection. It has become increasingly clear that the oral cavity can act as the site of origin for dissemination of pathogenic organisms to distant body sites, especially in immunocompromised hosts such as patients suffering from malignancies, diabetes, or rheumatoid arthritis or having corticosteroid or other immunosuppressive treatment. A number of epidemiological studies have suggested that oral infection, especially marginal and apical periodontitis, may be a risk factor for systemic diseases.
The teeth are the only nonshedding surfaces in the body, and bacterial levels can reach more than 1011 microorganisms per mg of dental plaque. Human endodontal and periodontal infections are associated with complex microfloras in which approximately 200 species (in apical periodontitis) (140) and more than 500 species (in marginal periodontitis) (97) have been encountered. These infections are predominantly anaerobic, with gram-negative rods being the most common isolates. The anatomic closeness of these microfloras to the bloodstream can facilitate bacteremia and systemic spread of bacterial products, components, and immunocomplexes.”
Recent research has identified that a significant proportion of brain abscesses may have their origins in oral including dental infections. “Dental infections have been implicated as the cause in multiple cases of brain abscesses and the recent death of a child in Boston. Reported dental sources of brain abscesses have included dental abscess, cellulitis, periodontitis, extractions, root-canal therapy, periodontitis, application of braces and osteomyelitis. (Link) (Link)
Everything is interconnected; oral and dental health is a marker of wider health including inflammation status, and a factor in its determination, with fundamental ramifications including in pregnancy;
“Mothers of preterm low-birth-weight infants and primiparous mothers of preterm low-birth-weight infants (n = 93) had significantly worse periodontal disease than the respective mothers of normal-birth-weight infants (controls). “(107)
All this brings us back to the central focus of Western Price’s later research how to minimise dental decay and optimise dental formation in the first place.
Fluoride – increasing numbers of cases of fluorosis in USA
The is no question that fluoride can harden enamel in the young, but may not commensurately improve the structural status of the underlying dentine.
Excess ingestion is a risk. I recently met a mother whose child had taken to eating toothpaste in the understanding that fluoride would help improve his teeth. Given the description of staining and crumbling molars, it is possible he was developing fluorosis. The side of a fluoridated tooth paste carton generally carries health warnings as to the dangers of ingesting the toothpaste presumably primarily due to its fluoride content.

The issue of fluoride is complex, and impacted by a number of factors including presence of other minerals in water / or fluoride containing foods / beverages. Fluoride is also present in pesticides and has other sources.
This graph come from the Fluoride Alert web site http://fluoridealert.org/issues/fluorosis/ . The Fluoride Alert site is full of thought provoking and informative material.

Photographs of Dental Fluorosis by Dr. Hardy Limeback and Dr. Iain Pretty, et al. (From the Flouride Alert Web Site)
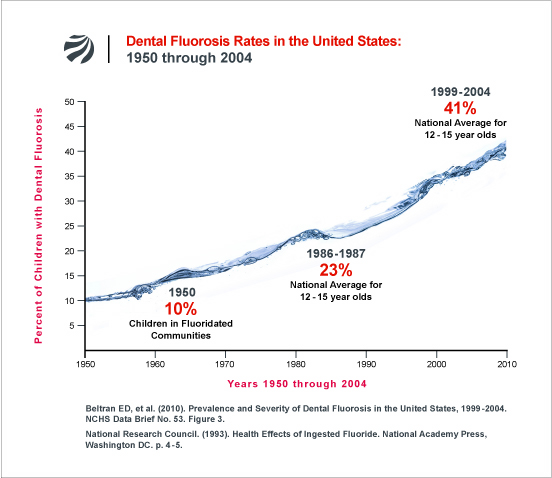
‘Flouride Alert’, an excellent information resource, takes a very strong position on fluoride addition to water: we take no position on that debate leaving the issue to others, but do recognise that excess of fluoride is a very real health issue. The amount of fluoride likely to cause problems likely varies according to other dietary factors, and mineral contents of waters.
However it is noted that breast milk appears to be very low in flouride (it appears to be excluded by body systems), and that flouride may cross the placenta and potentially negatively impact brain formation, (Link) which raises a need for research into the use of flouridated water or water containing natural flouride, for reconsititution of baby formula. Negative impacts of any excess of flouride will likely be compounded by low iodine. (Link)
“Fighting Dental Caries in Kids: Could Vitamin D Be the Secret Weapon?” says Colgate.
Their web page (link) starts 🙂
“Dental caries continues to be a prominent disease in children. According to Nutrition Reviews, past research studies have shown that dental caries in children can be reduced by up to 50 percent by increasing intake of Vitamin D. Recently these existing studies on dental caries reduction have been reexamined and show promise for the control of early childhood caries. These results indicate that Vitamin D could be a secret weapon in the battle against cavities in childhood and beyond.“
and included the observation 🙂
“ According to this systemic review, the benefits of Vitamin D introduced in childhood include the following:
- Improved tooth development
- Better formation of dentin with lifetime effects
- A topical protection similar to fluoride
- Changes in the amount and components of saliva that enhanced enamel strength
- Enhanced whole body immunity
The review also revealed a decrease in caries by up to 47 percent when Vitamin D supplementation was introduced. Also, recent studies looking at tooth development in utero and the effects of deficiencies in Vitamin D, recognized a link to enamel hyperplasia in children. Simply increasing Vitamin D during pregnancy and early childhood could give kids a better chance of fewer cavities and stronger bones.”
Prevention better than decay
It surely has to be better through diet to as far as possible optimise tooth formation in utero, and subsequently in early development, to prevent rather than treat tooth decay, and particularly so, given dental and oral infections can have much wider consequences because they provide an access route for bacteria into tissue, and so the wider body, with potential consequent involvement in many conditions including brain abscesses (link) and endocarditis (link).
The wisdom garnered in Western Price’s (Link) and the Mellanby’s (Link) work on the relevance of diet (including vitamin D) to dental formation and decay, and greater importance of it than dental hygiene, which itself is unquestionably important, still almost 100 years later, has not been taken fully on board.
Weston Price’s extensive work in the 1920’s on the potential spread of infection of dental origin, including potentially over time from root fillings, to wider tissues, and the impact on both general and specific tissues, is only just beginning to be more widely recognised.
Lack of timely application of such hard won knowledge and related societal inertia (Link), arguably due to lack of ‘commercial so human income generating related driving factors’, brings us back to the poignant plea of Dr Weston Price in the early 1920s, as to the need for application of such hard won evidence based knowledge.
 He was driven in his work by what must be at the apex of parental guilts, his deceased son died of focal sepsis, likely due to a root filling at presumably at his own hand. (Link)
He was driven in his work by what must be at the apex of parental guilts, his deceased son died of focal sepsis, likely due to a root filling at presumably at his own hand. (Link)