


Tuberculosis; an example of a widespread potentially fatal disease of bacteriological origin, currently treated with antibiotics.
We take the capacity of modern medicine, and in particular antibiotics, to cure bacterial based conditions such as tuberculosis for granted. We have forgotten how dreadful such conditions are, because they are now not commonly encountered. The reality is that antibiotic strains of tuberculosis are becoming more common, and treatment is becoming more difficult.
There is no question that antibiotic resistance is becoming a huge issue, both because of the over and miss use of antibiotics, and additionally because of the discharge of both antibiotic and antibiotic resistant bacteria in urine and faeces in sewage into the wider environment.
A study titled ‘Antimicrobial resistance in Africa: a systematic review’[i] reports “Internationally, there is a growing concern over antimicrobial resistance (AMR) which is currently estimated to account for more than 700,000 deaths per year worldwide [1]. If no appropriate measures are taken to halt its progress, AMR will cost approximately 10 million lives and about US$100 trillion per year by 2050”.50
[i] Tadesse B, Ashley E, Ongarello S, Havumaki J, Wijegoonewardena M, González I, Dittrich S. Antimicrobial resistance in Africa: a systematic review. BMC Infect Dis. 2017; 17: 616. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5594539/
These are massive and complex topics that take up rows of academic publications. The purpose of this page is simply to provoke thought as to the wider issues surrounding antibiotic usage and resistance, including the relevance and role of nutrition in health, by using tuberculosis as an illustration.
The aim is also to bring focus on the severity of such diseases, and so the consequences of inability to treat them if antibiotic resistance continues to increase, which absent significant action at many levels is likely.
It is also important not to overlook that susceptibility to disease in the prime as against end of life is in part a function of nutritional status.
Heliotherapy
A poster on the wall of the Wellcome Trust library. (see below)
In a world before antibiotics, good diet, fresh air and lots of it including sleeping outside, were the best available remedies for active tuberculosis, some improved many eventually died. Before antibiotics, the use of sunshine was an important genuine innovation and cutting edge treatment (likely benefit increased vitamin D – low vitamin D remains a major health issue and is associated with incidence and progress of tuberculosis). This both illustrates the importance of vitamin D and the lack of other treatment options before the development of antibiotics.
The burden on individuals society and national purses of a reemergence of more widespread resistant tuberculosis could be huge.
“Tuberculosis (TB) is a top infectious disease killer worldwide.
In 2014, 9.6 million people fell ill with TB and 1.5 million died from the disease.
Over 95% of TB deaths occur in low- and middle-income countries, and it is among the top 5 causes of death for women aged 15 to 44.” WHO (Link)
Tuberculosis once developed is a serious condition. The effect of TB on lung tissue is graphically illustrated in this cattle lung lesion dissection slide .(Link)
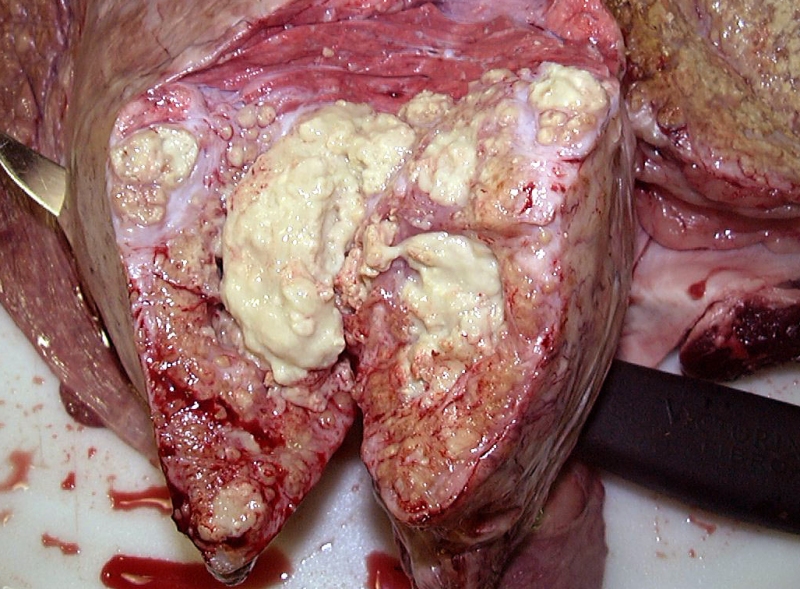 Tuberculosis lesions in the lungs of a two-year-old heifer. Courtesy of the USDA Food Safety and Inspection Service.
Tuberculosis lesions in the lungs of a two-year-old heifer. Courtesy of the USDA Food Safety and Inspection Service.
“Antibiotic resistance ‘could become bigger threat to mankind than cancer’“
Independent News Paper Headline 14-4-2016 (Link)
The latest evidence suggests 10 million people a year could die globally by 2050, as a result of antibiotics becoming powerless against common infections – more than currently die from cancer, he will say.”
Reasons for inclusion of the topic of antibiotic resistance on this site.
A brief discussion as to antibiotic resistance has been included for a variety of reasons including:
- Mellany, McCarrison, Weston Price, Trowel and others in their research into human health clearly observed availability of nutrients such as vitamin A and D impacted on susceptibility to and progression of disease including those that are microbial based.
- Albrecht and Howard identified the same principles applied to livestock, and the plants they feed on, and further that plants in turn depend on nutrients in the soil.
Healthy humans and livestock lower the need for antibiotics and other microbials so reducing the risk of resistance developing. Historical reports and modern research shows amenability to infections and disease, and subsequent treatment of them are dependent on nutritional status. For example fish oil, which used to contain all three, was an accepted and it would appear sometimes surprisingly effective treatment for active tuberculosis then called ‘scrofula’ (see below). These effects were reported by professional level headed doctors including in lengthy books on the subject of tuberculosis.
Huge numbers globally are now insufficient or deficient in basic ‘nutrients’ such as iodine, vitamin D, Omega 3s, which will inevitably impact susceptibility to infection and disease progression.
The development of resistance is a very serious matter. We have ‘forgotten’ how desperately unpleasant some bacterial related conditions including tuberculosis and syphilis are, how prevalent they have been at times during human history, and how limited treatment options (including historically use of mercury) were before the development of anti-microbials including antibiotics.
Other bacterial conditions include, tetanus, typhoid, cholera, plague, gonorrhea, Legionnaire’s, pneumonia, and anthrax. (Link)
Development
The discovery and development of antibiotics was a truly wondrous achievement allowing control of some very unpleasant and sometimes fatal conditions including but by no means limited to tuberculosis.
Resistance
Resistance is developing to many microbial treatments including antibiotics for a number of reasons as set out in a WHO report; “Antimicrobial resistance threatens the effective prevention and treatment of an ever-increasing range of infections caused by bacteria, parasites, viruses and fungi” and “is an increasingly serious threat to global public health that requires action across all government sectors and society” (Link).
One of the reasons cited is that antibiotics are or have been heavily used in an industrial food chain to promote grow and or facilitate large numbers of animal being reared at high densities in industrial settings.
In the 1960s following acceptance of the risk of the emergence of bacterial resistance in animals, it was agreed as a general principle that antibiotics should not be used for animals if useful in humans. A paper called “Effect of Abolishment of the Use of Antimicrobial Agents for Growth Promotion on Occurrence of Antimicrobial Resistance in Fecal Enterococci from Food Animals in Denmark” (link) states “Because of the emergence of multiply resistant bacteria causing infections in humans, some of these classes of antimicrobials have become important last resort drugs in the treatment of such infections. Examples include avoparcin, virginiamycin, and avilamycin, which belong to the same classes as the human drugs vancomycin, quinupristin-dalfopristin (Synercid), and evernimicin (Ziracin), respectively.“
It also states “Multiply resistant pathogenic bacteria have emerged worldwide during the last couple of decades, and multiple antimicrobial resistance is now one of the serious concerns of the new millennium” “It is unlikely that new antimicrobial agents can be developed at a rate to adequately combat the increasing number of multiresistant bacteria”
Related relevant resistance factors include methods of disposal of human ‘waste’ and the need to develop alternative technologies that allow safe return of the nutrients and organic matter in human urine and faces to the land
As mentioned development of antibiotic resistance is also greatly accelerated by the way we treat and dispose of human waste. Arguably there is a pressing need for a technological revolution in how we view human urine and faeces as a resources, how it is collected and processed, and it value as a resource to maintain fertile land so optimally healthy and nutrient dense crops.
McCarrison (link), Howard (link) and Albrecht (link) were all supremely aware of the centrality of well maintained soils to plant health, so livestock and human health.
Both antibiotic residues and antibiotic resistant bacteria are found in human urine and faeces. The current methods of collection and treatment of sewage are poor at removing both many pharmacological residues, and antibiotic resistant bacteria, which are in part eventually discharged in water courses. The risk of pollution by pharmacological residues, and development of antibiotic resistance is even greater where sewage treatment is minimal or non-existant.
A study looking at water samples in Africa concludes
“Some of the surface water is located in a very crowded location and near refuse dumps and pit toilets where they constantly receive doses of fecal materials possibly from pollution from human activity (septic tank, diving), pets, and wild birds.”[i] . . . “The antibiotic susceptibility studies showed that large proportions of isolates were resistant to sulphamethaxoid (SUL), cephalothin (CEP), tetracycline (TET), penicillin G (PEN), oxytetracycline (OXY), cefotaxime (CEF), nalidixic acid (NAL) and cefuroxime sodium (CXM).” “The presence of these multi-drug resistant strains in water samples could facilitate transmission of antibiotic resistance. This emphasizes the need for proper treatment of water in the study area.”
[i] Onuoha S. The Prevalence of Antibiotic Resistant Diarrhogenic Bacterial Species in Surface Waters, South Eastern Nigeria. June 2017Ethiopian journal of health sciences 27(4):319 https://www.researchgate.net/publication/318073833_The_Prevalence_of_Antibiotic_Resistant_Diarrhogenic_Bacterial_Species_in_Surface_Waters_South_Eastern_Nigeria
Example of an antibiotic treated bacterial disease – tuberculosis
An example of a bacterial disease is tuberculosis (Link), which is developing resistance to treatment. Current generations have never had the misfortune of witnessing the effects of diseases such as tuberculosis because treatments have largely been available.
Reality of Tuberculosis (as an example of a bacteriological condition)
 These Indian children were dying of tuberculosis, which took a very severe toll on those North American Indians whose diet included modern ‘western’ non-traditional foods. Weston Price (Link) ‘Nutrition and Physical Degeneration’ ch 6. fig.16.
These Indian children were dying of tuberculosis, which took a very severe toll on those North American Indians whose diet included modern ‘western’ non-traditional foods. Weston Price (Link) ‘Nutrition and Physical Degeneration’ ch 6. fig.16.
Tuberculosis “was the most common cause of death in the United States in the nineteenth century”.
 With thanks to Wikipedia (Link)
With thanks to Wikipedia (Link)
Fresh air including sleeping outside, good food, and in some clinics sunshine “helotherapy” were the only treatment options, as set out in this image courtesy of a UCLA article titled “Scourge of the City” (Link).
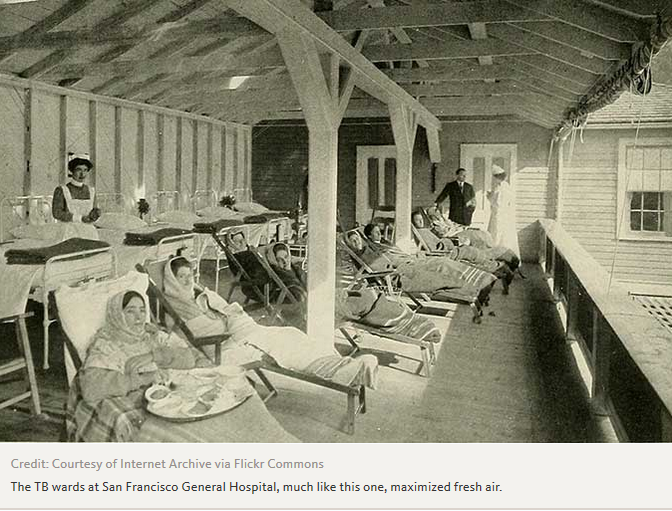 “Carried by the hordes eager to grab gold, tuberculosis began a frightening, infectious march through San Francisco in the mid-1800s. Known then as consumption, given the way it appeared to consume the body, or as white plague, given the ghostly pallor of its victims, the disease found a receptive new home in the wild West Coast city.“
“Carried by the hordes eager to grab gold, tuberculosis began a frightening, infectious march through San Francisco in the mid-1800s. Known then as consumption, given the way it appeared to consume the body, or as white plague, given the ghostly pallor of its victims, the disease found a receptive new home in the wild West Coast city.“
Pottenger Jr. (link) lost his mother to tuberculosis, and the Pottenger clinic provided treatment to people with lung conditions, in the days before antibiotics, when treatment options were extremely limited, and hence their driven interest in the power of diet to improve health including dietary experimentation on cats for 10 years.
A modern global perspective
Tuberculosis and antibiotic resistance is becoming a growing global health concern.
Role of Diet including vitamin D in reducing occurrence and development of disease including Tuberculosis
Diet including access to vitamin D was and is recognised in being a risk factor in transmission of and recovery from TB. (Link) Those observations of Swiss Doctors and all their patients, were not as cranky as some on seeing the poster above might think :). Many studies suggest a role for vitamin D in reducing the risk of incidence and or progression of tuberculosis. Vitamin D also has wider roles in immune function. Low vitamin D is a current and pervasive problem in large segments of poplations globally.
“Serum levels of vitamin D in TB patients are lower than in healthy controls (2,3). Paradoxically, prolonged treatment of TB also causes a decline in serum vitamin D levels (2)” (Link)
“Supplementation with high doses of vitamin D accelerated clinical, radiographic improvement in all TB patients and increased host immune activation in patients with baseline ‘Deficient’ serum vitamin D levels. These results suggest a therapeutic role for vitamin D in the treatment of TB.” (Link)
Iodine (additive to fish oil and improved diet) was suggested by reports in the early 1900s to be a useful treatment for certain categories of tuberculosis. (Link) Iodine insufficiency is seen in large numbers in 2018 in many countries.
Vitamin A is similarly linked to risk and progression of tuberculosis. “Vitamin A deficiency strongly predicted the risk of incident tuberculosis disease among household contacts of patients with tuberculosis.” (Link)
The lives of McCarrison, Mellanby, Weston Price, Pottenger, McCollum and others, were dedicated to looking at the effects of nutrients on the onset and prevalence of both communicable and non-communicable disease. They all concluded that adequate diets so nutrients were central to disease prevention, and deficiencies increased risk of occurrence.
I suggest it would be very difficult to read their research and not come to the same conclusion they did; that good diet will moderate the effects and risks of acquisition of a wide range of conditions, or as Hippocrates observed as an underlying principle “Let Food by Thy Medicine”.
Access to modern surgery and treatment should be a health bonus rather than a substitute for good diet and ‘sensible’ lifestyle.
Scrofula (non-lung tuberculosis often seen in the young) and fish Oil
Interestingly there are several reports in medial literature in the 1800s that fish oil mitigated the effects of and even in some patients was reported to cure scrofula.
Tradition fish oil used to contain vitamin A, D, some iodine and likely other fat soluble nutrients as well as Omega 3s. Modern refining strips out much or all of the A, D, and likely iodine. (Iodine is a recognised antibacterial (link)) Where stripped out the A and D are generally replaced by measured but lower doses.
The mechanism of action of fish oil on scrofula in the 1800s was not known. Today we know that nutrients act in synergy, that TB incidence is connected with poor nutrition and including low vitamin A and D. We also know Omega 3s and 6s and their oxidised products have many and often opposing physiological roles in the body. The effect of the nutrients in fish oil are likely to have been synergistic and cumulative where deficiencies were addressed.
Different reports suggest different efficacies for different forms of fish oil. The fish oil had different characteristics depending on whether it was the ‘virgin oil’ or that extracted by heat. The omega 3s and 6 fats are susceptible to oxidation. Oxidised products will likely cross the gut membrane and have bioactive effects. Omega 3 products include known anti-inflammatory products. Oxidised lipid products, particularly Omega 3s may have contributed to the curative properties of the fish oil due to increased intake of vitamin A, D and iodine. Much is still unknown about the effects of oxidised products of Omega 3 on human cellular function.
Fish Oil and Scrofula (references)
London Medical Gazette: Or, Journal of Practical Medicine, Volume 25 (Link)
The Medico-Chirurgucal Review, and Journal of Practical Medicine (Link)
TREATISE on the OLEUM JECORIS ASELLI, or, COD LIVER OIL,
as a THERAPEUTIC AGENT IN CERTAIN FORMS OF GOUT, RHEUMATISM, AND SCROFULA – 1847 – JOHN HUGHES BENNETT, M.D., F.R.S.E. (link)
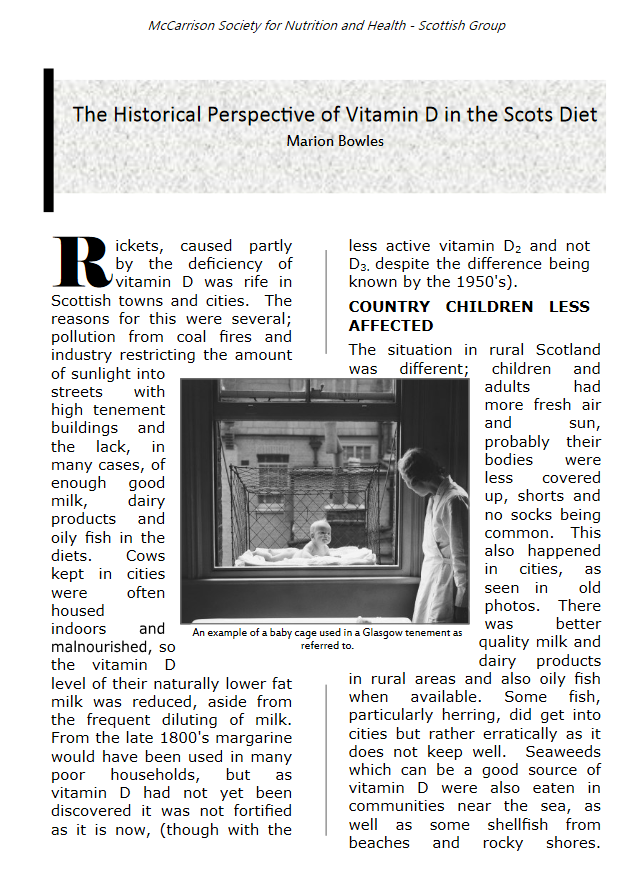
Historic public recognition of the importance of Vitamin D; window cradles in Glasgow tenements, and UV for children in Town Halls
 Heliotherapy, including exposure to sun, was commonly used as part of tuberculosis treatment. Clinics were set up in the alps, possibly because results were better due to higher UVB penetration at altitude.
Heliotherapy, including exposure to sun, was commonly used as part of tuberculosis treatment. Clinics were set up in the alps, possibly because results were better due to higher UVB penetration at altitude.
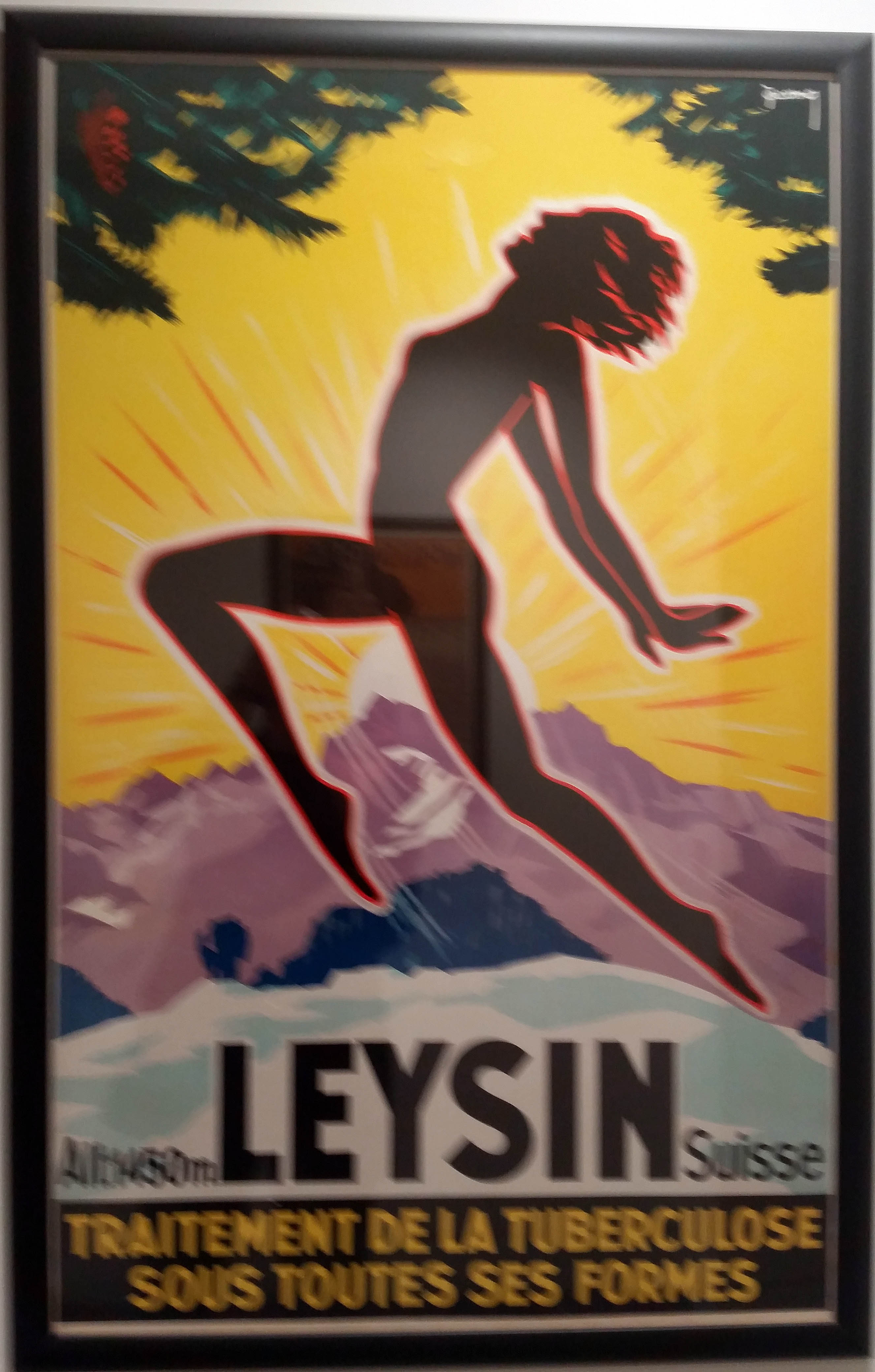 Poster on the wall at the Wellcome Trust Library
Poster on the wall at the Wellcome Trust Library
The public perception of the relative benefits and dis-benefits of non-burning exposure to sun has changed, and today significant number globally are insufficient or deficient in Vitamin D. (Link)
Relevance of diet to tuberculosis and other factors including UVB exposure – research by McCarrison Mellanby etc.
McCarrison, Mellanby, Weston Price, Pottenger, Sinclair and others, all in effect early researchers in deficiency diseases, from different positions all essentially took Sinclair’s (Link) position that nutrients were essential to cellular function so health:
“The deficiency of any nutrient which is essential for every tissue will eventually lead to abnormal function in every tissue. That is so incontrovertibly obvious that I am continually astonished by the eminence of the medical scientists to whom it must be forcefully restated.”
“The second is that when deprivation of an essential nutrient occurs, not all tissues will be simultaneously and equally affected, and not all individuals will react in the same way. Which tissue shows symptoms first will depend on the genetic inheritance of the individual and on his or her exposure to environmental factors and lifestyle events.”
They realised that pathways were interlinked and synergistic, and that absence or excess of a particular nutrient may impact on the requirement for another.
They noted that well fed study animals were more resistant to a range of conditions and that one or more individual nutrient deficiencies could be associated with the onset and progression of particular conditions.
In the commercially driven race, to understand biological pathways often for the purposes of creating commercial products, we have arguably lost sight of the ability of diet to moderate disease, and more particularly of the insufficiency or deficiency or particular nutrients such as vitamin D and iodine to exacerbate, even lead to, the onset of a wide range of debilitating, socially ‘costly’, as well as ‘expensive’, medical and health related conditions.
Paraphrasing the words of Dr Burkitt in the admirable quest to improve our capacity technology and expertise in medical ‘mopping floors’ of disease, we should not forget we need also to turn of the taps of disease. (Link)
Curative medicine does not prevent disease.
Healthier people have less need of antibiotic treatment.