


|
The Saccharine Disease Conditions caused by the Taking T. L. CLEAVE, M.R.C.P. (Lond.) Member of the Institute of Linguists Preface THE term, ‘refined carbohydrate foods’, will be shortened in this work to ‘refined carbohydrates’. The mass incrimination of these, especially sugar and white flour, over many of the ills of Westernized countries today, was first advanced by the author of the present work in a long paper in 1956; [1] and as far as he knows he was the first to advance this unitary conception, which he later promulgated under the term, ‘the Saccharine Disease’. [2] The original paper included the chart now given in Chapter II, showing the enormous rise in sugar consumption over the last century and a half, and the conditions blamed on this consumption, and on that of white flour, included diabetes, coronary disease, and obesity; peptic ulcer; constipation, haemorrhoids, and varicose veins; Escherichia coli infections such as appendicitis, cholecystitis, pyelitis, and diverticulitis; together with renal calculus, many skin conditions, and of course dental caries. Later the author published monographs on coronary disease, varicose veins, and peptic ulcer and carried the conception further forward, especially in the last named work; and later still in a joint work. [3] In the present volume, then, which is the author’s final elaboration of his conception, and which draws on his previous publications, and also on his contributions to the joint work just mentioned, it will be contended that the causation of all the foregoing conditions has been obscured through an insufficient distinction being drawn between the consumption of unnatural, refined carbohydrates, like sugar and white flour, and that of natural, unrefined carbohydrates, like raw and dried fruit and wholemeal flour. Thus, while the consumption of all carbohydrates may not be rising appreciably with the rise in incidence of a condition, the consumption of refined carbohydrates may be rising very strongly indeed. Once the distinction between the two consumptions is sufficiently appreciated, it is contended that the causation of all these conditions can be exposed, the mechanism of disease production usually being quite a simple one. From this it is argued that all the conditions discussed are really the manifestations of a single master-disease, the understanding of which disease is held to be of decisive importance to the Westernized nations, so that a large amount of suffering and disablement can be prevented and in many cases alleviated. The author considers that the most accurate name for the master-disease referred to is the ‘Refined-carbohydrate Disease’, but because the main refined carbohydrate involved is sugar, and because the starch from white flour is converted in the body into sugar, he has, as already stated, introduced the term ‘Saccharine Disease’, which is a much more convenient one. The word ‘saccharine’, meaning ‘related to sugar’, should, however, follow the Oxford English Dictionary and be pronounced like the river Rhine, so as to distinguish it sharply from the word for the chemical sweetener, which is pronounced ‘saccharin‘ or ‘sacchareen‘. A feature of the present conception is simplicity, and though the author himself considers this to be a most important indication of correctness, it by no means follows that such simplicity favours rapid acceptance by others. On the contrary, medical minds throughout the world these days seem so preoccupied with detail that perhaps sometimes they fail to exercise the practice of repeatedly standing back in order to view things with greater perspective, which enables them to be explained more simply. As a consequence, obvious common-sense conclusions may be lost sight of in a mass of detail or missed altogether. It was not always so. Nearly 2500 years ago the Greeks had already realized that one of the most important of empirical facts is that correct explanations are nearly always simple explanations. There is a fragment (176) in Aeschylus, from the last play, that says so (‘for the words of truth are simple’), and the same thing is stated in Euripides, Phoenissae, circa 469: which became proverbial throughout Greece. Whether the correctness of simple explanations stems from the scientific contention that the whole Universe is an expression, in endless combinations, of a single ultimate reality, variously termed the mass/energy unit, etc., does not call for discussion here, but the author is so persuaded of the empirical link between simplicity and correctness in explanations that he has a certain sympathy for some people, who practise the habit of mentally submitting to a great-grandmother their answers to difficult problems — if these answers make sense to her, they derive confidence from it. This is also in line with the expressed belief of one of the great architects of modern nuclear physics, the late Lord Rutherford, that if a theory is any good, it should be understandable by an ordinary barmaid. In the author’s opinion, provided always that one keeps strictly within the limits of naturalness — that is, within the limits set by human evolution — the danger of oversimplification is incomparably less than that of overcomplication. We must seek the ‘positional play’ of Chess. It does not follow, alas! that trying to reach the truth through thinking simply is easy. On the contrary, the author submits that thinking things out in terms of simplicity is far harder than thinking them out in terms of complexity. Indeed the latter procedure tends to be only too easy. Nor does it follow, if true explanations are nearly always simple, that simple explanations are nearly always true. Incomplete, or incorrect, possession of the facts may render the latter contention very far from being the case, and is the usual cause of ‘oversimplification’. This book, then deliberately aims at simplicity. It must also be emphasized that the present conception has to be presented here in stark outline, with the minimum quantity of references, for the number of disease conditions involved precludes a convincing presentation in any other manner. In the earlier joint work the author’s conception of a single saccharine disease was accompanied by Dr. G. D. Campbell’s excellent racial studies in diabetes and coronary thrombosis, which strongly supported these parts of the conception. In the present much-extended presentation of the conception these studies can only be referred to, but they invite pursuit in the earlier work and in the original references. Dr. Campbell has also edited a recently published work Clinical Medicine in Africans in Southern Africa (Livingstone). The author is deeply indebted to his friend, Dr. Kenneth Vickery, for many years of sustained help, as the last chapter will clearly show; to the late Mr. Arthur Elliot-Smith and to Dr. Walter Yellowlees for their graphs on appendicitis, together with much other friendly assistance; to Sir Richard Doll and to Mr. Denis Burkitt for the invaluable support they have given to this conception, and without which it would scarcely have survived its birth; to Mr. Laurence Knights for his shrewd observations based on a surgical experience that embraces both England and Africa; and last, but far from least, to his wife for her unfailing judgement and good advice. Finally, if this book has a future, he hopes that Dr. Kenneth Heaton, of the next generation to the author’s, will have a say in it, for he has supported the conception from an early date and given the author the benefit of some fruitful conversations, as referred to in Chapter XI. References1. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 42, No. 2, 55. 2. — (1962), Peptic Ulcer. Bristol: Wright. 3. — and Campbell, G. D. (1966), Diabetes, Coronary Thrombosis, and the Saccharine Disease, 1st ed. Bristol: Wright. (2nd ed., with N. S. Painter, 1969.) Chapter IThe Law of Adaptation. Hereditary Defect. Personal Make-upTHIS work is based on human evolution, and stemming from it the perfect adaptation of all species to their natural environment. It is to be recalled that it was this adaptation, universal in extent and profound in degree, that excited the imagination of Darwin from an early date, and it was actually on his explanation for it — the struggle for existence, with survival of the fittest — that his theory of evolution was primarily based. Various explanations had been offered in the past for this adaptation, which had excited the imagination of others long before Darwin, but none so logically linked the adaptation with the time factor as his did. This latter factor is likewise of great importance to the present work, where the necessity will be stressed of an adequate period of time for adaptation to take place in a species to any unnatural (i.e., new) feature in the environment, so that any danger in the feature should be assessed by how long it has been there. It is fortunate that though there may still be differences of opinion over exactly how adaptation in species takes place, there are none over the fact that it does take place, for it is only with the latter fact that we are concerned here. The adaptation to their environment which is constantly taking place in all species, and which at times has attained stages bordering on the miraculous, will be referred to in these pages as the ‘Law of Adaptation’, an expression that will be found to confer many advantages. Hereditary Defects The law of adaptation is not absolute. Nature — that is to say, a 3000-million-year span of evolution — has not led to completely perfect adaptation in an organism to its natural environment, and evolution is still taking place. Hereditary defects, therefore, do occur. Normally the struggle for existence, i.e., the evolutionary process, keeps these failures very rare indeed. It is a matter of common observation that amongst wild creatures commonly consumed as human food, such as herrings, rabbits, or wood-pigeons, any hereditary defect (‘congenital malformation’) is a very great rarity. In Man, however, under civilized conditions, these defects have been allowed to become more prominent. Even under these conditions, however, the struggle for existence has prevented the rate of any hereditary defect exceeding 5 per 1000 live births, the highest rates being the following: [2,3]
It follows from the above that before postulating an exception to the law of adaptation and attributing an ailment to a hereditary defect, the frequency of occurrence, or incidence, of the ailment should be considered. If the incidence is many times as great as that of any known hereditary defect, then, quite apart from other considerations, such a cause for the ailment becomes extraordinarily improbable. For example, in the case of some of the conditions to be studied here, such as varicose veins and peptic ulcer, the incidence is over twenty times as great, which makes hereditary defects as the cause of them correspondingly untenable. This approach by incidence-figures is thus of great value in deciding whether a disease is due to a hereditary defect, or to a new factor in the environment to which no adaptation is yet possible — in short, to use a commonplace expression redeemed by its clarity, in deciding whether the body is built wrongly or is being used wrongly. And this distinction is itself of great value in deciding the all-important question of treatment. For if the disease is due to hereditary defect — i.e., if the body is built wrongly — the only treatment possible will be either operative repair or some form of replacement therapy; whereas if the disease is due to a new factor in the environment — i.e., if the body is being used wrongly — the treatment is at once directed to the removal of the cause. The two types of treatment are utterly different. Another subject of great importance that falls for discussion now is personal build or make-up. These terms are used here to cover the healthy personal variations that occur in any part of the body, including even the smallest structures. Because of the inclusion of even the smallest structures, ‘personal make-up’ will normally be the term used. (The author prefers these terms to others like ‘phenotype’, ‘constitution’, etc., which nowadays are likely also to cover environmental influences, [4] which is exactly what he does not intend here.) The reason why this subject is so important is that a person’s healthy make-up may interact strongly with a new environmental factor, and any resulting disease will then require very careful differentiation from a hereditary defect, since, though healthy make-up and defect are poles apart, they are equally hereditary. This is best made clear by some examples. Consider, first, the infantry assaults against enemy entrenchments in the First World War of 1914-18. In that war it was found, as would be expected, that during these assaults tall men were shot down by machine gunners considerably more often than short men were. Yet no one looking at a tall man killed in this way would have considered the death due to a hereditary defect in the structure of his body, since in natural circumstances the tallness might have been an advantage, not a disadvantage. No: the basic cause of death clearly lay in the new environmental factor of fast-travelling bullets, to which no adaptation could yet exist and to which this man’s personal build made him especially vulnerable. Consider, again, the case of hallux valgus. In this condition a hundred pairs of feet can go into shoes that are too pointed, and yet only ten of them, say, will develop the hallux valgus deformity. These feet have no structural defect! Far from it: unconfined by shoes they might, in fact, be particularly efficient in certain natural circumstances, such as on long marches or during jumping from one piece of rocky ground to another. But the personal make-up of these feet, though perhaps particularly helpful in the foregoing circumstances, happens also to make them particularly vulnerable to the new environmental factor of pointed shoes — so new a factor that even today only a small fraction of humanity goes about in shoes at all, let alone in pointed ones. And it is this new factor in the environment, to which no adaptation can yet exist, and to which the make-up of these feet renders them especially vulnerable, that is clearly the basic cause of hallux valgus. These considerations show the enormous distinction that exists between a disease due to a hereditary defect in the body and one due to an unnatural, that is to say new, factor in the environment to which a person’s build or make-up renders him especially vulnerable. The distinction is not only a big one — it is also a crucial one. For once again it constitutes the difference between the body being built wrongly and being used wrongly, with its vital bearing on the type of treatment to be pursued. Thus, in the case of hallux valgus above, one’s attention is directed primarily to the shoes, not the feet. It will be noted that terms like ‘susceptibility’ to a disease do not properly distinguish between make-up and defect, as set out above, and will therefore particularly be avoided in this work. Heredity It follows from what has been written that the presence of hereditary features in a disease may, during a search for the cause of the disease, become a snare and a delusion, owing to make-up being just as hereditary as defect. And if make-up is what is involved, hereditary features in this are utterly unimportant. For example, what does it matter, in the case of the tall man mentioned above, if his father was also tall and was killed in a similar manner in the Boer War? Or if the person with hallux valgus had a parent with a similar type of foot, which, confined in pointed shoes, also developed hallux valgus ? In such cases discussion of hereditary features in personal make-up not only becomes waste of time, but also may act as a red herring drawn across the trail. For it may distract the attention from the only thing that matters — the removal of the cause, in the shape of the new environmental factor. This distraction of the attention at the present time is seen only too clearly in the diseases to be studied here. In the differentiation between personal make-up and hereditary defect in the causation of a disease, one is guided by the incidence-figures of the disease, the date of onset, and the presence or absence of certain clinical characteristics, based on developmental details (e.g., the fusion of embryonic planes, etc.). There is seldom any difficulty, but in a doubtful case racial studies may be conclusive, as in those undertaken here. Such are the evolutionary considerations on which this work is based, and their value will be seen throughout the work. With regard to the term ‘Nature’, as used above, it may be added that there is nothing unscientific, and much that is convenient, in this term, provided it is realized that it does no more than personify the total span of evolutionary adaptation on this planet. So compact an expression will therefore be made use of from time to time and much space thereby saved. References1. Park, W. W. (1964), Lancet, 2, 579. 2. Grundy, F., and Lewis-Faning, E. (1957), Morbidity and Mortality in the First Year of Life. A Field Enquiry in Fifteen Areas of England and Wales. London: Eugenics Society. 3. Carter, C. O., and McKeown, T. (1961), personal communication. 4. Brock, J. F. (1972), Lancet, 1, 701. Chapter IIConception of a Single, ‘Saccharine Disease’I. General ConsiderationsAS stated in the Preface, there will be advanced in this work the conception of a single, ‘saccharine disease’, due to the consumption of refined carbohydrate foods, and with various manifestations in individual persons dependent on personal make-ups in the parts of the body affected. The conception of this disease did not dictate the evidence for it — the evidence dictated the conception, as will be readily seen from the facts set out in the following chapters. But it is nevertheless desirable at the present moment to consider the conception from a different point of view — the evolutionary one. Of all the foods that exhibit an alteration from the natural state, the refined carbohydrates — represented in this country chiefly by sugar and white flour — exhibit the greatest. In the former approximately 90 per cent of the sugar-beet or sugar-cane has been removed, and in the latter 30 per cent of the wheat has been removed. Furthermore, it is to be noted that these alterations are so recent by evolutionary standards of time as to date but from yesterday. It is true that, apart from earlier evidence from Egypt, white flour was being produced in Greece at least as early as 500 B.C., and Hippocrates himself recommended white bread for diarrhoea, which shows that it was already realized as passing through the gut at reduced speed. [1] Furthermore, a quotation from Antiphanes, written before 350 B.C., shows that bakers were by that time producing white loaves in quantity, and in A.D. 50 the production of white flour was geographically widespread, though socially confined to the higher grades of society in all the countries producing it. [2] In Britain, from the time of the Roman occupation, the flour was ever more frequently sieved to remove the bran, but even at the end of the sixteenth century white bread had not yet appeared in the cottages of the poor, though by the end of the seventeenth century some of the poor were eating it. However, at the end of the eighteenth century [3] practically all the poor were eating white bread, and so the turn of that century — i.e. around the year 1800 — is an approximate baseline, as it were, for the dating of general white flour consumption in this country. And as regards sugar (which in this book means, unless specified as occurring in raw fruit or other natural foods, the ordinary white and brown table sugar sold in grocers’ shops), Fig. 1 shows the extraordinary recentness of the alteration, in which a consumption in this country of about 15 lb. per head per year in 1815 has risen to about eight times this figure — i.e., to about 120 lb. — today, over 150 years later.
Contrast in both particulars the practice of cooking food, which not only involves a relatively trifling alteration in its constituents, but also, as regards the time factor, is of an antiquity to match the discovery of fire itself, some half a million years ago. [4] Consequently, we are now well-adapted to the practice of cooking. As set out in an earlier work [5] referring to the saccharine disease, the refining of carbohydrates produces its very harmful results in three main ways:
The third of these mechanisms will be discussed later, in Chapter X, on peptic ulcer, but the second mechanism, itself based on the first, calls for considerable amplification at this point. The over-consumption, as stated, stems from the concentration present in refined carbohydrates, which concentration not only deceives the taste buds in the tongue, so that they cannot signal accurately enough when to stop eating these foods, but also interferes with the normal distension of the stomach and hence with the feeling of satiety. This is all easily perceived if eating a small quantity of sugar, say roughly a teaspoonful, is contrasted with eating the same quantity of sugar in a natural form, such as exists in an ordinary apple. A person can take down teaspoonfuls of sugar fast enough, whether in tea or any other vehicle, but he will soon slow up on the equivalent number of apples. No deception takes place with these. The argument can be extended to contrasting the 5 oz. of sugar consumed, on the average, per head per day in these islands with up to a score of average-sized apples, or with a large sugar-beet weighing some 2-1/2 lb., in which this quantity of sugar approximately is present. Who would consume that quantity daily of the natural food? Or if he did, what else would he be eating? Much of the rise shown in Fig. 1 stems from this cause. In the case of white flour the concentration that has been produced is less than in the case of sugar, and so the over-consumption that results is less, too; but that over-consumption does result can readily be seen if eating light, puffy, white bread is contrasted with eating the heavier, denser article represented by a true wholemeal bread. The fact that the rising consumption of sugar during the last century has been accompanied by a falling consumption of (predominantly white) flour does not permit the exoneration of the latter. Such alteration in consumption merely exchanges some of the damage inflicted by the flour for the still greater damage inflicted by the sugar — and there remains the damage inflicted by the amount of white flour still being consumed. II. The Refining of Flour and Sugar, and the Relative Dangers of the Two1. Evolutionary Considerations As regards which of the two refined carbohydrates, white flour (starch component of) and sugar, is the more dangerous, we must first state that the main difference between the two is a quantitative one. Qualitatively, both starch and sugar end up in the body as glucose, though we shall amplify this statement later, but quantitatively the refining processes concentrate the sugar some eight times as much as they concentrate the flour, and therefore evolutionarily the sugar emerges as much the more dangerous of the two, being that much more removed from the natural state. For it is the unnaturalness that governs the deception of the tongue and appetite, and therefore the danger of over-consumption. a. The Refining of Wheat Although white flour was being generally consumed in this country by the year 1800, as stated above, it is a fact that around the year 1880 the introduction of steel rollers into milling practices enabled a still whiter flour to be produced (70 per cent extraction instead of 80 per cent extraction). It is very important that the relative consequences of this innovation should now be assessed, for on it might be blamed the emergence of the saccharine disease. Let us therefore examine the innovation in detail. Now it is a crucial fact that in the milling of grain the fibre (bran) is not removed evenly from the grain as the degree of milling increases. The fact is, as the author has pointed out, [6] that the fibre in grain is placed mainly on the outside of the grain, to protect it from injury, just as a hard shell protects the underlying nut. Therefore, the fibre in grain is mainly removed in the earlier, lighter degrees of milling. This is beautifully shown in Fig. 2, modified from the diagram in the book entitled Bread by Lord Horder, Sir Charles Dodds, and T. Moran, [7] which reveals that a flour containing even as much as 90 per cent of the original grain has already lost most of its fibre (bran). Indeed, the same diagram shows that the steel-roller mills of 1880 only removed an extra 9 per cent or so of the fibre already removed by the old stone-grinding mills. In the case of Canadian wheat, the figure of 9 per cent is reduced to only 6 per cent — and twice as much Canadian wheat is used in the United Kingdom as English wheat. Meanwhile, at around the same date the consumption of refined sugar was rising by leaps and bounds, as seen on the sugar chart (Fig. 1).
b. The Refining of Sugar It could still be contested, however, that although sugar consumption was rising so strongly at the above period, it was not displacing an equivalent consumption of the natural parent sugar-cane or sugar-beet. This is true, but the displacement took place by proxy. Let this be demonstrated by a few simple examples. As the sugar gets more concentrated, so it becomes more exciting to the taste. For example, red currants on a bush are moderately attractive, but a good red-currant jelly, containing, as it does, added sugar, is much more attractive. And there lies the trouble! How can the young people of this country today, forever chewing some concentrated sweetmeat, be expected to seek out those natural analogues that, in more primitive circumstances, would be so desirable to them? Even such sweet fruits as the banana appear rather dull by comparison, and as for sweet vegetables like the parsnip — who on earth wants to be bothered with things like parsnips any more? How many apples would be eaten at a pop festival, by comparison with ices and sweetmeats? Nor must it be forgotten that, through the agency of evolution, the body’s instinctive desires for proteins, fats, and carbohydrates, though varying in individual persons, still bear to some extent a natural ratio to each other in any one person. If, then, the desire for carbohydrates is neutralized by the taking of concentrated sweetstuffs, it will not only be sweet fruits and vegetables that undergo a fall in consumption, but also potatoes and various grains, for the starch in these eventually ends up in the body as sugar, too, and so affects instinctive carbohydrate desires. And even some refined grains, let alone the humble potato, have more fibre than refined sugar, which has no fibre at all. Hence the above argument on refined sugar versus refined flour still holds, even though it chiefly holds by proxy — by sugar-displacement of other, less concentrated, carbohydrate foods, such as bread. We now come to what is considered here to be the decisive consideration in assessing the relative dangers of white-flour consumption and sugar consumption — the results of restitution. If the experience of the present author counts for anything, who introduced the unprocessed bran into human therapeutics 40 years ago [8] and has been employing it — often on a very large scale — ever since, the replacement of the present white loaf in the diet of Westernized countries by the pre-1880 white loaf, both qualitatively and quantitatively, would make only a negligible difference to average intestinal transit times. People who were constipated before would remain for practical purposes just as constipated still. This he considers as certain as anything in this life can be. But what is even more important, the introduction of a true wholemeal loaf into Westernized diets like our own, with its average sugar consumption of some 5 oz. per head per day, would by no means restore natural transit times, either. The transit times would be improved, certainly, and people who were constipated would experience some relief — but not a decisive relief. As long as the sugar-displacement of fibre, described above, remained, no true relief would ever be obtained. To that statement, too, the author unconditionally commits himself, and he submits that were it not correct, the seven million aperient-takers in this country, to be referred to later, would long ago have switched over to wholemeal bread of themselves. Increasing the consumption of fibre by the taking of additional bran, especially of the unprocessed type, to compensate for the fibre displaced by sugar is another matter and would certainly do the trick, as the saying is, over transit times. * * * But alas! this is not the end of the story. For so far we have only been discussing the direct effect of fibre on the gut, in which the fibre, or bran, derived from grain is invaluable, but when we come to discuss the indirect effect of fibre, in controlling over-consumption, the picture changes at once. This is because, though the bran would certainly correct the over-consumption from eating white flour, it would signally fail to correct the over-consumption from eating sugar — which is far the more serious over-consumption of the two. The reason for this failure is partly because the fibre present in most fruits and sweet vegetables is much bulkier than the fibre or bran derived from grain, and therefore satisfies the appetite much more effectively; but mainly because the desire for sweetness is one of the strongest of desires where food is concerned, and unless the fibre is allied naturally to sugar, as in fruits and sweet vegetables, so that this desire for sweetness is neutralized, the correction of the over-consumption from eating sugar will seldom be achieved — most people will just break the rules and eat sugar or foods containing sugar, such as chocolate. Anyone can take the bran and prove the foregoing for himself. These considerations, together with the fact, as will be set out shortly, that the conditions caused by over-consumption, such as obesity, diabetes, and coronary disease, are even more serious than those arising directly from the loss of fibre itself, show very clearly that sugar is far more dangerous to the human body than is even the whitest of flour. In order to deal successfully with over-consumption and with the dental conditions, it will be imperative not only to substitute wholemeal bread for white but also substantially to substitute natural sweet things for sugar, such as raw fruit, sweet vegetables, and certain dried fruits, like figs, raisins, and currants, as set out in the diet card at the end of this book. Trying to do without sugar often fails, but the above natural substitution for it can be very successful, and should be carried out to the limit the purse can afford. Such a procedure also usually renders superfluous the taking of any additional bran. Indeed an aphorism becomes possible here: ‘In anyone taking a true wholemeal flour, the need for taking unprocessed bran as well is roughly proportional to his or her consumption of (refined) sugar.’ Finally, taking sweet-tasting chemicals like saccharin is rejected here as a solution to the problem of over-consuming sugar. Quite apart from possible dangers in the prolonged taking of this coal-tar derivative, there is also the important question of depriving the body of a class of foodstuff (sugar) which, as already said, is desired for its taste almost more than any other, and which in its natural form must therefore be of very great value. Such a step, it is submitted, would be an example of trying to be clever at Nature’s expense, i.e., at the expense of evolutionary adaptation. The author, himself, would rather take a small amount of sugar. Furthermore, a low blood-sugar, i.e. hypoglycaemia, might result in faints and motor accidents in certain people. III. A Further Note on BreadAlthough the author of the present work has for many years incriminated refined sugar to a far greater extent than refined flour, as shown above, he could never agree with Professor J. Yudkin that a preference for brown (wholemeal) bread over white bread, based on nutritional grounds, is akin to ‘colour prejudice’. To the author, wholemeal bread, quite apart from its crucial biochemical advantages, especially in fibre, stands for natural nutrition and for health, whereas white bread stands for unnatural nutrition and the degenerative diseases. To many peoples on this globe bread (or rice) is still the staff of life, and to these peoples the distinction between the two types of bread (or of rice) could spell the difference between life and death. But even to those peoples (and especially to those individual persons) to whom bread is not the staff of life, the difference is still one of very real importance. Furthermore, those who deliberately stick to the natural or evolutionary path over bread, and those who carelessly depart from it, are very likely indeed to do the same over other foods. The choice of bread is therefore doubly significant. The author is well aware of the argument commonly heard, that the missing substances in white bread can always be replaced from other foods. But can they, in practice? Let us look into this assertion more closely. First of all, how many people know how to make this replacement? Second, how many people can afford to buy the necessary amounts of fruit and vegetables, where the fibre is infinitely more expensive than it is in wholemeal bread? Thirdly, in the case of old people, how many can find the energy to forage for these foods, living as they often do in some little old top room on their own? The present author stands firm on the supreme importance in personal and national nutrition of eating a true wholemeal bread. Experience has taught him how dangerous it is to try to be clever at Nature’s expense, as already referred to. IV. Statistics on Fibre-LossIt has been argued that there has been no fall in the fibre-content of the British diet over the last 100 years, [9] and, from what the author has presented above, it is clear that most cereal fibre was lost by the year 1800, and much of the sugar-displaced fibre was lost before the year 1890, when the consumption of sugar was nearing present exalted levels. So it is true that comparatively little extra fibre has been lost over the past 100 years. (The situation in the United States would be quite different, owing to the fall in maize consumption, as set out in Chapter III. No maize is eaten in the United Kingdom.) But this makes no difference to the conception presented in this book. For the saccharine disease has been with us on a big scale from the beginning of the present century (i.e. for the last 70 years), and some of its manifestations from long before that; furthermore, it will shortly be seen that the incubation periods of its manifestations extend in some cases up to 40 years, so that even an unchanged fibre-loss over the last 100 years, as now under discussion, would be amply accommodated by the conception. But in truth no one, it is submitted, can really know what the fibre-loss has been over the last generation, let alone over the last 100 years. Even a generation ago allotments were common and gardens were prized; many vegetables and soft fruits were cultivated. Today allotments have largely been built over and it is easier to sell a house without a garden than with one; there is far less cultivation of vegetables and fruits. How many people go blackberrying in the countryside today compared with this common event years ago? One cannot be guided too much by Board of Trade returns; the whole tenor of our lives has altered and is still altering — and with it has altered the personal cultivation of vegetables and fruits, for the consumption of which no statistical records can exist. But all this is idle talk compared with the medical realities today, which comprise inter alia the present enormous sale of aperients, to some seven million people in these islands alone, as will be shown later; and the immediate relief from this state of affairs by the restitution of the fibre lost through the consumption of sugar and white flour. We are not really concerned, either here or anywhere else, with the uncertainties of the past, but with the clear indications of the present. We must judge by results, today. V. Qualitative Considerations in the Consumption of Sugar and White FlourThe reason why little allusion has so far been made to qualitative differences, as opposed to quantitative differences, in the consumption of sugar and white flour, is that though the starch in white flour is digested to and absorbed as glucose, whereas sucrose (i.e. ordinary table sugar) is absorbed as fructose as well as glucose, these qualitative differences are natural ones and therefore have little claim on our attention compared with the highly unnatural quantitative differences so far described. In this connexion it is to be noted that many fruits abound in fructose, as the word indicates. In amplification of the above, although the starch in flour yields glucose on digestion, whereas (table) sugar (sucrose) yields fructose as well as glucose, and although the metabolic pathway of fructose in the body is different from that of glucose, the conversion in the blood-stream of fructose into glucose (assuming the fructose is taken in natural amounts, as opposed to experimental amounts) is so rapid that this difference between glucose and fructose becomes of little practical importance. This is shown, for example, in the usual failure to substitute with advantage fructose for glucose in most clinical treatments (e.g. in diabetic coma). [10] We therefore come back to the quantitative difference between white flour (being less refined) and (table) sugar (being more refined) already carefully discussed, and in this connexion Swan, Davidson, and Albrink [11] have shown how much faster is the digestion and absorption into the blood-stream of (table) sugar than the starch in flour (partly owing to the presence of other and impeding materials in the latter case, like the protein present in flour); and it will be seen in Chapter VII, on diabetes, that it is the speed of the glucose impact, not its size, that upsets the evolutionary adaptation in the pancreas and is held here to cause the disease. Similarly, starch and (table) sugar lead to different degrees of change in the lipids and other constituents of the blood, but these changes cannot be pursued here. VI. The Main Manifestations of the Saccharine Disease, in Relation to the Taking of Refined CarbohydratesWe now come to what the author, after many years of thought, plus trial and error in practice, considers is the correct assignment of disease to the loss of fibre, over-consumption, and loss of protein, respectively, that were described at the beginning of this chapter as the three main consequences of the refining of carbohydrates. The grouping given is not always to be considered absolute — for example, in the E. coli conditions the effect of over-consumption on the bacterial proliferation in the intestine is aggravated by the stasis caused by loss of fibre. Nor are all the conditions involved set down in this grouping, as will be elaborated later.
The separation of the manifestations into groups in this manner is not merely a matter of convenience, but also has a direct bearing — via clinical associations — on aetiology and treatment. For though there is a loose clinical association between all the manifestations of the saccharine disease, the manifestations in one group (i.e., caused by one mechanism) are naturally much more closely associated with each other clinically than with those in another group (i.e., caused by another mechanism). For example, it will be shown in later chapters how closely associated with each other are the conditions due directly to loss of fibre, such as intestinal stasis, diverticular disease, haemorrhoids, and varicose veins; and in later chapters, too, how closely associated are the conditions due to over-consumption, and only indirectly to loss of fibre, like obesity, diabetes, and gall-stones. The best paper known to the author on the latter associations (i.e., those stemming from over-consumption) is that by M. D. Kaye and F. Kern. [12] Even these iconoclasts admit a probable clinical association between obesity, diabetes, and gall-stones. The author himself, and others whose studies have been widely reported, would put it much more strongly than that; and he would also add coronary disease to this group, which Kaye and Kern also propose should be added, but the association of which they do not regard as proved. However, at least the crucial association of coronary disease with diabetes now appears to be very generally accepted, and will be elaborated on later in this work. These clinical associations clearly throw much light on aetiology. [13] For example, it will be shown in Chapter VIII, on coronary disease, that with the close association between this disease and diabetes, and with the strongest reasons for believing diabetes to be caused by over-consumption from the taking of refined carbohydrates, and only indirectly caused by the loss of fibre in these carbohydrates, it is reasonable to consider the same cause for coronary disease itself. But the separation of the manifestations into the groups set out above bears directly on treatment, too. [13] For the adding of unprocessed bran to the diet, as described earlier (and later), will have a magical effect on conditions like constipation, haemorrhoids, and diverticular disease, but little or no effect on obesity and diabetes. For the first group, being due directly to loss of fibre, is alleviated by the restitution of any type of fibre; but the second group, being due to over-consumption and only indirectly to loss of fibre, is alleviated by the restitution of fibre only to the extent that this corrects over-consumption, not only of flour but also of sugar, as already explained. Thus, in the writer’s opinion, it would be as futile to try to arrest coronary disease with bran as it would be to try to arrest latent or early diabetes with bran (or, for rather different reasons, to arrest dental decay and periodontal disease). A type of fibre restitution which also corrects sugar consumption is absolutely essential in conditions like these, and bran supplies neither the bulk nor the natural amount of sugar needed for success. The type of restitution needed is, indeed, set out in the natural-diet card at the end of this work, as already stated. It may be added here that the importance of over-consumption (especially of sugar), as distinct from direct loss of fibre, in the production of many manifestations of the saccharine disease, is well seen in the explosive outbreak of this disease now taking place in the Canadian Eskimoes, following on their sugar consumption passing 100 lb. per head per year. This has recently been set out in a comprehensive manner, [14] and it will be seen later that dental caries, appendicitis, diabetes, and gall-stones are now rampant amongst these people, and in the author’s opinion other manifestations (especially coronary disease) will certainly follow. But it is impossible to explain these events by much loss of fibre. For the natural diet of these Eskimoes has always been conspicuously lacking in fibre, which has seldom exceeded the fibre found in the faeces of the reindeer, sometimes eaten by them as a vegetable during the summer months, and the fibre found in bilberries, also eaten at that period. (In the natural Eskimo diet the chewing of raw meat replaced the effects of fibre on the teeth and gums, and the eating of seal fat largely replaced the aperient effects of fibre on the intestines; for practical purposes no sugar was eaten.) In fact, the Eskimoes pursuing a sophisticated existence today consume far more fibre — from the eating of tinned fruits and certain vegetables — than ever they did in their natural existence. Yet, as said, many manifestations of the saccharine disease are now becoming common to them, which shows the much greater importance of over-consumption in the production of many saccharine manifestations. And since sugar is by far the most refined carbohydrate, it is in sugar that this over-consumption is always most conspicuous and most in need of correction. And the same applies, though in a slightly different manner, in dental decay and periodontal disease. VII. The Question of Proteins and FatsTo turn now to the other two main classes of food, whilst proteins are rarely appreciably altered from the natural state, it is true that some fats, such as butter and certain vegetable oils, show a very large alteration, and indeed a concentration comparable to that produced in the refined carbohydrates. But the concentration here never seems to deceive either the tongue or the appetite, and the reason for this, in the author’s opinion, is that fat in Nature often occurs in pure form, such as the fat in meat. For instance, butter and margarine contain about 85 per cent fat, whereas, to give an example of the fat in meat, the perinephric fat (suet) in oxen and sheep contains about 99 per cent fat. The result is that the tongue and the appetite are evolved to cope with the consumption of pure fat and no over-consumption occurs. Thus, no more fat would be consumed in the case of bread and butter or bread and margarine, where the fats have been concentrated artificially, than in the case of bread and dripping, where the fat is equivalent to the pure fat in beef, that can be cut off with a knife and shows no concentration at all. Certainly a person’s tongue is a very sensitive guide indeed to his fat requirements, whatever type of fat is involved. Some people are Jack Sprats, who can eat no fat, and some are the opposite. In close accord with all this, the rise in fat consumption per head in the Westernized nations over the last century or so has probably been only about 25-50 per cent. [15, 16] Indeed, M. A. Antar and others have recently shown that total fat consumption in the United States has increased by only 12 per cent over the last 70 years, [17] and similar figures have been collected by B. Friend. [18] To sum up, then, there is no doubt, from an evolutionary point of view, that, in any disease in man due to alterations in his food from the natural state, the refined carbohydrates, both on account of the magnitude and the recentness of the alterations, are always the foods most likely to be at fault, and not the fats. It will be seen in the following chapters that the incrimination of the refined carbohydrates on evolutionary grounds is supported by equal incrimination on epidemiological grounds, and the conception of a single saccharine disease is thus based on two independent foundations. VIII. Harmlessness of Unrefined CarbohydratesThe conception set out above, of mankind not being adapted to the consumption of refined carbohydrates, must be carefully distinguished from that advanced by J. Yudkin, [19] that the human body is not properly adapted to the consumption of unrefined (i.e. natural) carbohydrates either, because ‘with the discovery of cereals some ten thousand years ago, man for the first time became a food producer and ceased to rely on gathering and hunting his foods’. The present author cannot accept this view, for three separate reasons. Firstly, he does not hold that man until ten thousand years ago was primarily a carnivore. To quote from H. M. Sinclair’s [20] objection to the same view: ‘When man first started to keep his forepaws off the ground he ate fruit, nuts, and berries, as do the apes to-day; he could not kill and eat woolly rhinoceroses without fangs or claws. When he had tools he hunted and ate animals, including himself, but in the Chellean and Acheulian epochs he was probably vegetarian, apart from gathering grubs.’ However, exactly what man ate in bygone ages must be largely conjectural; what is not conjectural is the structure of the human body today, which indicates with much clarity that man is further from being a pure carnivore than from being a pure herbivore. Though in fact omnivorous, he is, as Sinclair states, most typically a frugivore or fruit-eater — which is much closer to the herbivore than the carnivore. Thus man lacks the carnassial teeth for tearing flesh, and the rasping tongue of the carnivore (though he also lacks the specialized molars of the herbivore). His saliva contains the ferment, ptyalin, for digesting starch, characteristic of the herbivore, whilst his gastric juice, also like that of the herbivore, contains only a fraction of the hydrochloric acid present in the carnivore. There is not the least doubt that man is fully equipped to live on plant foods, as indeed many hundreds of millions of rice-eaters in China, India, and elsewhere abundantly reveal today. Secondly, Yudkin’s conception implies that man cannot rely on his sense of taste when eating foods in their natural state — i.e., that his sense of taste may be evolved out of harmony with the rest of his body, so that he may like eating whole cereals or other natural carbohydrates without being able properly to metabolize them. But logic dictates that the body is evolved harmoniously, as a whole; and so does the evidence, too, for a herbivore, like a horse, will die of starvation rather than eat meat or other animal foods, which it cannot metabolize; whilst a carnivore, like a lion, will die of starvation, too, rather than eat grass or other plant foods, which it likewise cannot metabolize. Thirdly, and most important of all, it will be the endeavour of this work to show that all the manifestations of the saccharine disease discussed are strikingly absent in those races still subsisting almost exclusively on just these unrefined carbohydrates. In this connexion it is to be noted that the occurrence of diseases like kwashiorkor, common in eaters of grain, like maize, even when eaten unrefined, in no sense indicates any lack of adaptation in the body to the consumption of these grains. The truth is that man cannot live exclusively on any one type of foodstuff, and if he tries to do so, he suffers from a deficiency of the other types. Kwashiorkor occurs in those who live on maize and other grains — but on practically nothing else. It is a deficiency disease, and it would be as illogical to relate it to lack of adaptation to these grains as it would be to relate scurvy, occurring on a pure meat diet, to lack of adaptation to meat. And as regards the rare cases of allergy to (usually recently introduced) carbohydrate foods, it is submitted that these would be still rarer in the absence of the arbitrary food mixtures described in Chapter X. It is considered, then, that unrefined carbohydrates, including the starch in cereals and tubers, and the sugar in fruit, sugar-beet, and sugar-cane, are absolutely safe to eat in their natural state, and that trouble only arises when they are eaten after being refined from that state. One or two small exceptions are discussed in Chapter X. The distinction between these two views is fundamental, and has a direct bearing on treatment, as will be seen in all the conditions (including even obesity) to be discussed in this work, where the aim will always be to eliminate the refined carbohydrates, never the unrefined, natural carbohydrates. IX. Incubation Periods in the Saccharine DiseaseIt is important to remember that it takes time for the consumption of refined carbohydrates to produce the various manifestations of the saccharine disease. In short, these manifestations have incubation periods, which differ in each case. In some manifestations the incubation period is very short. Thus, a massive dose of sugary material could cause so great a proliferation of intestinal organisms that in some E. coli conditions, such as appendicitis (especially in children), the incubation period could be a matter of hours, and it will be seen later that sweetened dummies can cause the destruction of all the milk teeth from decay in a matter of months. But it will also be seen that in the case of diabetes the incubation period may be 20 years, in the case of coronary disease 30 years, and in the case of diverticular disease 40 years. It is clear that the incubation periods of the various manifestations will depend partly on the degree of concentration (refinement) present in the carbohydrates consumed (sugar, for example, being considerably more concentrated than white flour, which, as will be shown later, makes it especially important in the causation of E. coli conditions, like appendicitis); partly on the amounts of such carbohydrates being consumed, and partly on different personal make-ups in different persons and even in different races. It is also clear that the incubation periods in single persons may differ from those in whole communities or whole countries. Thus, if in a country the large-scale refining of flour long precedes that of sugar, then conditions that can follow the refining of flour, such as haemorrhoids, may well precede those more intimately related to the consumption of sugar, such as the appendicitis just referred to, even though the personal incubation periods are the other way round. When evaluating, therefore, the epidemiological evidence for or against any given medical condition being a manifestation of the saccharine disease, it is clearly most necessary to look into the various aspects of the incubation period, especially in conditions like coronary disease, where the period can be a very long one. It is clear that the long incubation period in most saccharine manifestations can render present personal appearances very deceptive. Thus, as regards R. A. McCance’s and E. M. Widdowson’s [21] well-known trial with German schoolchildren after the last war, one group fed on wholemeal bread and another on white bread and with both groups apparently in much the same state of health at the end of a year, these two groups could well have had very differing medical futures if they had carried on with their two different breads in later years. To take, perhaps, the least serious example, would a bigger proportion of the white-bread children have eventually joined the great army of aperient-takers today? To judge by the present rapid spread in Great Britain of the taking of unprocessed bran for constipation, this could well have proved to be the case. And the pathway of intestinal stasis is littered with conditions like haemorrhoids, in the earlier stages of the pathway, and like diverticular disease, in the later stages of the pathway. And as regards over-consumption, would a bigger proportion of the white-bread children have eventually joined another great army of people — those who are over-weight? To judge by the admitted importance of very small amounts of over-consumption, if repeated day after day, year in and year out, this could well have proved to be the case too. And the pathway of obesity is littered, as we have seen, with even more serious conditions than is the pathway of stasis. And what about peptic ulcer? When one remembers the ulcer belt of India, in which the population takes milled white rice instead of home-pounded brown rice, as will be seen in a later chapter, can it be excluded that, in spite of the greater diversity of food over here, a bigger proportion of the white-bread children would not have ended up with this complaint also? X. Final ConsiderationsWith regard to the groups of conditions advanced above as due to the consumption of refined carbohydrates, and together comprising a single saccharine disease, it is considered here that when any one of these conditions occurs without apparent reason, i.e., idiopathically, as is normally the case, there is no other basic cause for it than the consumption of these unnatural foods, though other, modifying factors may well be present. Far from it being difficult to believe that there is but a single basic cause for any of these conditions, it is suggested that what would be difficult to believe would be the exact opposite — that there were multiple basic causes for it. In fact, in the author’s opinion, when such multiplicity of causes is advanced, the less likely are any of them to include the right one. It is noteworthy, for example, how, by increasingly general consent, the primary cause of dental caries has gradually been narrowed down to the single one given here, and he is confident that in due course the same sequence will take place with the other conditions listed. Nor does he consider it an improbability that the same primary cause should exist for many separate conditions, and that such attribution shows loss of perspective. On the contrary, he holds the very opposite to be the case — that it would be an extraordinary coincidence if these refined carbohydrates, which are known to wreak such havoc on the teeth, did not also have profound repercussions on other parts of the alimentary canal during their passage along it, and on other parts of the body after absorption from the canal. Indeed, just in the way that, as the knowledge of syphilis widened, conditions such as aneurysm of the aorta and general paralysis of the insane, which originally were never imagined as connected with the disease, gradually became added to ft as systemic manifestations, so, as the author advanced in the joint work in 1966, may this be true of the saccharine disease, which logically should involve many systems, too. For it is much more logical that a single cause, the consumption of refined carbohydrates, like the single cause of arsenic poisoning, for example, should be regarded as resulting in a single disease with many systemic manifestations than in a whole lot of separate diseases. Distant HorizonsThe above approach points to possible new advances in the understanding of causation, and also in treatment. Thus, thyrotoxicosis appears to be a very possible saccharine manifestation. It is known to be rare in tribal Africans, but seems to be getting commoner in certain urban areas, such as Nairobi. [22] This is the classic march, both temporal and geographical, of a saccharine condition, as Western foods are introduced into primitive communities. The clue could be worth pursuing, as it would explain why, in the author’s experience, the natural, unconcentrated diet appears to be beneficial in early cases of thyrotoxicosis. Similarly, there are certain aspects of disseminated sclerosis, involving sugar consumption, [23] that suggest it may be a saccharine manifestation in the central nervous system, but these aspects cannot be pursued here. Likewise schizophrenia might represent a different type of involvement of the central nervous system, affecting the mind. The author can well imagine some astonishment on the face of the reader, but he would like to quote a personal communication from Dr. G. Daynes, of the Transkei region of South Africa, dated September, 1971: ‘Regarding mental disease in the people of the Transkei, I can say that in the past 11 years I have not diagnosed a single case of schizophrenia in a tribal African living on an unrefined carbohydrate diet, whereas this disease is the commonest psychosis among the urbanized Africans. The “School people”, who come in between the tribal and the urbanized, have an appreciable incidence of the disease, but they consume considerable quantities of white sugar and refined maize-meal, leading to a high incidence of obesity and a small but increasing incidence of diabetes.’ It may be added to this that schizophrenia in the U. S. Negro is as common as in the white. [24] Meanwhile, the profound stasis in the bowel so notorious in cases of melancholia lends some credence to the possibility that schizophrenia may be implicated in the saccharine disease, too. What would be the mechanism of production in the speculative manifestations suggested above, if they proved eventually to be realities? The author believes it could lie in each case in the absorption of toxins from the intestines. Indeed, he finds himself gravitating more and more to Ehrlich’s conception of an intestinal toxaemia, referred to in Chapter IX, with the toxins, however, never forming as Ehrlich thought they did, under natural conditions, but only as the result of over-consumption through the taking of refined carbohydrates, and the bacterial putrefaction to which this leads (Chapter IX). The author might add that his gravitation to a modified Ehrlich conception, given above, stemmed partly from logic and partly from clinical experience in treatment. Such toxins in the intestine could also have local implications in the causation of Crohn’s disease and ulcerative colitis, which on temporal and on geographical grounds appear to have a very good chance indeed of being saccharine manifestations. [25] One thing is very clear: in any degenerative condition of unknown causation, the adoption of the natural, unconcentrated diet appears to be strongly indicated on general principles. The author has sometimes been blamed by his friends for resisting modifications in his conception. The reason for this does not lie, he hopes, in his getting older these days, but in the fact that he applied the conception in practice, not only widely in temperate and tropical climates but also for some 20 years as a physician in naval hospitals, before publishing anything. Therefore, with this prolonged clinical testing behind him, though the author believes that extensions to the saccharine disease will be made in the future, he does not believe that any appreciable modification of the present outline of the disease will be able to be sustained against it. He attaches great importance to the diet card presented at the end of book and the simple mechanisms behind it. We now turn our attention away from all speculative manifestations of the saccharine disease and direct it to those manifestations about which the author believes there is no doubt whatsoever. References1. McCance, R. A., and Widdowson, E. M. (1956), Breads, White and Brown, 9. London: Pitman Medical. 2. Ibid., 6. 3. Ibid., 46. 4. Clarke, W. E. Le Gros (1950), History of the Primates, 2nd ed. London: Trustees of the British Museum. 5. Cleave, T. L. (1962), Peptic Ulcer. Bristol: Wright. 6. — (1972), Brit. Med. J., 2, 409 7. Horder, Lord, Dodds, Sir Charles, and Moran, T. (1954), Bread. London: Constable. 8. Cleave, T. L. (1941), Brit. Med. J., 1, 461. 9. Robertson, Jean (1972), Nature, Lond., 238, 291. 10. Woods, H. F., and Alberti, K. G. M. M. (1972), Lancet, 2, 1354. 11. Swan, D. C., Davidson, P., and Albrink, M. J. (1966), Ibid., 1, 60. 12. Kaye, M. D., and Kern, F. (1971), Ibid., 1, 1228. 13. Cleave, T. L. (1972), Brit. Med. J., 1, 678. 14. Shaefer, O. (1971), Nutrition Today, 6, No. 6, 8; and personal communications. 15. Stone, R. (1934), Measurement of Consumers’ Expenditure and Behaviour in the U.K. 1920-1938. London: Cambridge University Press. 16. Keys, A. (1953), J. Mt Sinai Hosp., 20, 119. 17. Antar, M. A., Ohlson, M. A., and Hodges, R. E. (1964), Am. J. Clin. Nutr., 14, 169. 18. Friend, B. (1967), Ibid., 20, 907. 19. Yudkin, J. (1963), Lancet, 1, 1335. 20. Sinclair, H. M. (1963), Ibid., 2, 43. 21. McCance, R. A., and Widdowson, E. M. (1954), Medical Research Council Report, 287. 22. McGill, P. E. (1971), Brit. Med. J., 2, 679. 23. Roberts, H. J. (1966), Lancet, 4, 745. 24. From information kindly supplied for the author by Charles V. Menendez, Charity Hospital, New Orleans, October 1971. 25. Leader, Lancet (1972), 2, 942. Chapter IIIThe Saccharine Disease and the ColonIN this chapter the author will take the first consequence of the refining of carbohydrates, which is loss of fibre (pulp), and will trace the effects of this loss on the intestines. It has already been set out in Chapter II that the loss of fibre in the refining of sugar is greater than in the refining of flour, and therefore the effects of fibre-loss will — as in all manifestations of the saccharine disease — be more serious in the case of sugar consumption than in the case of white-flour consumption. As regards the effects of this loss on the intestines, especially the colon, nearly everyone knows that the more fibre (‘roughage’) taken in the food, as in the form of fruits and vegetables, the more satisfactory becomes the action of the bowel. The loss of fibre occasioned by switching from these natural foods to sugar and white flour has the serious contrary result of intestinal, and more particularly colonic, stasis, as we shall now see. First of all, what is the natural transit time of the intestinal contents? Following a letter to the British Medical Journal by the author and G. D. Campbell, [1] and through the kind co-operation of J. P. Bostock, radiologist to the Eshowe and Empangeni Hospitals in Zululand, Natal, and of W. E. G. Butler of the latter hospital, as arranged by Dr. Campbell, some pilot radiological studies were made on tribal Africans eating an unrefined diet, [2] and the figures obtained indicated (it is believed for the first time) that the natural transit time in the human intestines may be around 24-48 hours as against 48-96 hours or longer in Westernized countries. [3] In short, the unrefined diet halves the ‘normal’ transit times. Recently Burkitt, Walker, and Painter [4] have made comprehensive studies that indicate some, but not a serious, revision of these figures, the transit times with the unrefined diets still averaging less than half those with the refined diets. I. Simple ConstipationAs the result of the loss of fibre now under consideration, simple constipation is so common in these islands today that Medical Research Council observers [5, 6] have estimated that at least 15 per cent of the population are taking regular purgatives. Before discussing the easiest and cheapest way of correcting this state of affairs, it is desirable to pursue a further development of what has been set out above. II. Diverticular DiseaseThis term covers two conditions, diverticula of the colon (‘diverticulosis’) and inflammation of these diverticula (‘diverticulitis’). It may be added for the sake of clarity that until fairly recently the term ‘diverticulitis’ has very commonly been used for both conditions, it being assumed that the diverticulitis is a development and complication of a pre-existing diverticulosis. The author will argue here that both conditions stem from the refining of carbohydrates, though the mechanism in each is different. a. Diverticulosis It has long been considered that colonic diverticula may arise through excessive muscular contractions in the colon, which have the effect of raising the internal colonic pressures, thus forcing the lining mucous membrane to herniate through the muscular wall itself; and as a leader in The Lancet [7] Put it some years ago: ‘It is tempting to relate these abnormal pulsion forces to the unwise sophistication of a Western diet, that eschews roughage, since there is some evidence that the condition is becoming more common. C. Wells [8] commented on the remarkable freedom from diverticulosis in Africans eating a high-residue diet; and A. J. Carlson and F. Hoelzel [9] found that while a low-residue diet encouraged the formation of diverticula in rats, the addition of roughage prevented their development.’ In short, a postulated sequence in the production of diverticulosis is a refined diet leading to a slower passage of the colonic contents, which slowing leads to increased absorption of water and hence to greater viscosity in these contents, with consequent excessive contractions in the colon in its efforts to move the viscous contents onwards. A clear relationship of diverticulosis to a progressive refining of the diet might, in the author’s opinion, have emerged much earlier had it not been that in all investigations the control subjects without the condition were on the same refined diet as the subjects with the condition, so that personal make-up, as described in Chapter I, entered the aetiological picture to a confusing extent. Let us examine two examples of this. As long ago as 1925 Spriggs and Marxer, [10] in an investigation of 100 patients with diverticular disease, found that half the patients complained of constipation, and that of the remainder, who did not complain, many were also constipated; but they also found that 100 control patients without the disease were even more constipated. Likewise, Manousos, Truelove, and Lumsden [3] more recently showed that the intestinal transit times in subjects with this disease were accelerated rather than delayed, compared with control subjects without the disease. However, it is crucial to the author’s argument, as set out in the foregoing letter, [1] that these control subjects were taken from a population that was itself on a refined Westernized diet, in whom constipation has just been shown to be exceedingly common. Indeed, the control subjects showed retention of barium in the gut 3, 4, 5, or even more days in 90 per cent of the cases. Now it is easy to understand, as was, again, set out in the letter referred to, that the transit times in subjects with diverticular disease may be shorter than these times, because the condition is held here to be due, in certain people, to excessive muscular contractions in the colon designed to correct just this type of delay, but this is fundamentally different from the transit times in diverticular disease being shorter than the natural transit time set out above. On the contrary, they are certainly much longer than this time. To sum up: the difficulties in the past over relating diverticular disease to a refined diet appear to have been largely due to insufficient studies in persons on an unrefined diet. This latter aspect of the subject will shortly be extended to cover the historical and epidemiological features of the disease. b. Diverticulitis Although the inflammatory changes in diverticulitis are normally regarded as secondary to blocking of the exits of the diverticula, the author does not believe that this is fundamentally the case. The question of the bacterial population of the gut has also to be considered. It is to be noted that duodenal diverticula never progress to a diverticulitis, yet one could visualize that their exits also could at times become obstructed, in spite of the more fluid contents of the duodenum; is this freedom from infection connected with the sterile nature of the duodenal contents, due to the bactericidal powers of the gastric acid? The subject will be pursued in Chapter IX, on Escherichia coli conditions, where, although stasis is freely conceded as sometimes a factor — for example, in appendicitis — a much bigger factor is held to be the swarming of bacteria in the gut on a food surplus (especially a sugar surplus) that, with the consumption of naturally dilute, unrefined carbohydrates, would never be present. The subject will also be raised later in this chapter when discussing the conditions (especially diabetes) associated with diverticulitis. All that need be said at this point is that the greater importance of sugar consumption than of white-flour consumption with regard to loss of fibre in the causation of diverticulosis, already noted at the beginning of this chapter, is greater still with regard to over-consumption in the causation of diverticulitis, owing to the specially serious effects of sugar on the bacterial population in the gut, as will be set out in Chapter IX. In the past, in place of the view based on bacterial proliferation, just given, the view has been that coarse particles in the food led to blocking of the exits of the diverticula, and thus to the supervention of diverticulitis. That view has led for many years to a refined diet being prescribed for the condition — the very diet that is held here to be responsible for it. Epidemiology and History Proceeding now to the epidemiological and historical aspects of diverticular disease, it may be stated that both show a clear light on the causation. Thus, it is quite easy to establish that Africans living tribally on an unrefined diet (such as unrefined maize) do not get the disease at all. Indeed, the surgical superintendent of the Charles Johnson Hospital in the Zululand Reserve of Natal, South Africa, Mr. Anthony Barker, to whom the author has been indebted in his works for so much valuable information, stated in a personal communication in 1965 that no case of diverticular disease had ever been seen in that hospital. It is possible to compare this absence with the increasing frequency of the condition in Africans pursuing an urbanized existence, but, as in peptic ulcer, varicose veins, and other manifestations of the saccharine disease, the author has always preferred to try to establish comparisons with the Negroes in the United States, since these exhibit a much greater, and a much longer, deviation from the unrefined tribal diet than do their African cousins who have taken to the towns. In this quest he expresses his gratitude to D. D. Kozoll of the Cook County Hospital, Chicago, who in 1965 sent him the following personal communication: [14] ‘We see every complication of diverticulitis with equal frequency in the Negroes and the whites. We would cite a reference to you by E. J. Kocour in 1937, in the American Journal of Surgery, 57, 433, in which he comments on the rarity of diverticulitis in the U.S. Negro. However, you will notice that the reference goes back nearly 30 years, and the picture has changed since then.’ Following the receipt of this key reference, the author tried to ascertain changes in the diet of American Negroes since those earlier days, and it transpired that in the past century they largely subsisted on ‘hominy’, which consisted of unrefined maize, just as their African cousins when living tribally largely do today. But during the past century, largely through replacement by refined cereals (and refined sugar), the consumption of maize in the United States — in spite of the great increase in the population has shown a spectacular fall, as Table I reveals.
Turning now to the United Kingdom, as a country typical of Westernized civilization, it may be stated that though references to diverticula and diverticulitis occurred intermittently throughout the past century, and though these diverticula were related by some to the abnormal pressures in constipation, as set out above, they were always regarded as a rarity and were not described in textbooks of medicine. Like some other conditions constituting the saccharine disease, such as duodenal ulcer, which likewise was not described earlier in any textbook of medicine, diverticular disease emerged as an increasing clinical reality around the turn of the present century, i.e., around the year 1900, and has received growing attention ever since, in keeping with the rapidly rising incidence (so that a third of our population over the age of 60 now have diverticulosis [3]). The epidemiology and history of diverticular disease, both in Westernized and primitive societies, have recently been succinctly presented by Mr. Painter and Mr. Burkitt, [12] but the author cannot agree that the rising incidence of the disease owed much to the introduction of the steel-roller flour mills around the year 1880. As explained in Chapter II, very little extra fibre was lost through this development, and a far more significant factor is considered here to have been the steeply rising consumption of sugar at this period. Indeed, the curve in Fig. 1 (Chapter II) shows that, in the 20 years straddling 1880, sugar consumption in the United Kingdom showed the remarkable rise from about 50 lb. to about 80 lb. per head per year, which in the author’s opinion is of much the greater significance. For not only is more fibre lost in the refining of sugar, but also the effect of sugar on the bacterial population in the gut, as already set out, is of decisive importance. In any case, if the rising incidence of diverticular disease had been mainly due to the refining of the flour, it would have happened decades earlier, as by the year 1800 nearly everyone was eating white flour of 80 per cent extraction (see Chapter II). Incubation Period From epidemiological observations, including necropsy and clinical studies ranging from the past century to the present day, it would appear that the incubation period in diverticular disease is about 40 years. [12] That is, it needs some 40 years’ exposure to a typical Westernized, refined diet before the fully developed disease presents itself Clearly, this fact has to be carefully borne in mind in all research on the causation of the disease, especially with regard to evidence from primitive communities moving on to a Westernized diet. It was many years ago that the author first came to relate diverticular disease (or diverticulitis, as the condition was then commonly called, as stated above) to the taking of refined carbohydrates; and indeed it was in 1945, when appointed to the R.N. Hospital, Chatham, that he started treating such cases on this basis, including not only the prescribing of a diet rich in fibre, but also the prescribing of unprocessed bran, where he drew on his experience with this material over the previous 15 years, shortly to be described. At Chatham he had the good fortune to work with Surgeon Commander E. T. S. Rudd, F.R.C.S. (now Surgeon Rear-Admiral E. T. S. Rudd, C.B., C.B.E., F.R.C.S., whose co-operation here I have much appreciated), who was on the surgical side of the hospital and had every sympathy with this approach. Indeed his surgical colleague was himself a sufferer from diverticular disease and achieved salvation over this disease from the taking of the bran. In his original paper in 1956 [13] the author therefore included diverticular disease in his conception and likewise in 1966, in the first edition of the joint work, [14] where he set down ‘that the whole probable sequence of diverticulitis is in harmony with the view that the condition is a manifestation of the saccharine disease. For the removal of fibre in the refining of carbohydrates is not only responsible for the stasis that leads to diverticulosis, but also, via over-consumption, for the abnormal numbers of B. coli present in the gut, the attack of which bacteria on the wall, in the diverticular areas of stagnation, constitute the final diverticulitis.’ At this stage the author would again like to pay a tribute to Mr. N. S. Painter to whose support since 1967 he has been greatly indebted. [15] Mr. Painter’s experimental investigations in diverticular disease have been given in the second edition of the joint work, [16] and will now be outlined here. These investigations [17, 18] were made by using open-ended polythene tubes, which measure the intra-colonic pressure accurately (previous work with intra-colonic balloons is suspect, as it has been shown that ‘such balloons measure the pressure in the balloon and not the pressure in the lumen of the bowel’). These tubes were passed into the sigmoid colon through a sigmoidoscope, which was then withdrawn and the intra-sigmoid pressures were recorded, both in healthy subjects and in patients with diverticulosis. This pressure-recording was combined with simultaneous cine-radiography, which showed that when pressures were produced in the sigmoid colon, the colon was contracting so as to become demarcated into segments. This segmentation was due to the contraction of inter-haustral muscle rings, which probably occur at fixed sites in the colonic wall. By stimulating the colonic musculature with morphine and other drugs it can be shown that this segmental type of contraction can under certain circumstances generate pressures as high as 90 mm. Hg, and it is easy to see that in these circumstances diverticula of the mucous lining can be forced through the muscular wall. These studies clearly form an important step in understanding the production of diverticula in the colon, but the present author does not, if he may say so, consider that a narrowed state of the colon, which has been greatly emphasized in connexion with the effects of segmentation, would favour the development of diverticula, for he believes that the necessarily thicker colonic wall in the narrowed state would more than counterbalance the effect of the narrowing. He believes, on the contrary, that it is distension of the colon by the unnatural accumulations in stasis, and the resulting thinner state of the colonic wall, that favours the production of diverticula. With a natural diet the greater bulk in the food eaten likewise produces some colonic distension, but now any thinning of the wall is more than compensated by the much faster transit time and big fall in viscosity. Later, of course, when the damage is done, the wall thickens from infection. In connexion with a narrowed state of the colon in rats on a refined (low-residue) diet, Carlson and HoelzeI [9] in their phrase, ‘more or less’, do not rule out intermittent accumulations occurring in the colons of such rats, which the author would regard as inevitable for the reason given below. Certainly he is convinced that with a refined diet the colon in man is often in a more, not less, distended state than is natural. For to the drier contents of yesterday (and very likely of some days before that) must be added the moister contents of today, and this accumulation constitutes an addition, not a subtraction! Indeed, what does the term ‘loaded colon’ mean if it does not mean just this? That is why the author, himself, has always believed that the increase in viscosity of the colonic contents, so typical of stasis, is the decisive factor in the production of diverticulosis. Clinical Associations The subject of the clinical association between the conditions constituting the saccharine disease has already been alluded to in Chapter II, but here attention will be drawn to those associations involving diverticular disease, which are deeply revealing. Some of the associations noted in the past have recently been contested [19] but in a recent paper Parks, [20] reviewing 521 cases of diverticular disease, found the following associated conditions: appendicitis 14 per cent, cholecystitis and/or gallstones 13.8 per cent, abdominal hernia 12.5 per cent, duodenal ulcer 10.9 per cent, and dysentery 1 per cent. All these conditions could be included in the saccharine complex, if the abdominal hernias were related to straining at stool, due to stasis, and if the dysentery signified an irritable colon, shortly to be described. Recently, Mr. Conrad Latto [21] has demonstrated a most significant association with varicose veins, which had a doubled incidence in diverticular disease patients. It will be noted that in the past no attempt has been made to differentiate associations with diverticulosis from those with diverticulitis. Yet if the author’s conception is correct, a condition like abdominal hernia should be particularly associated with diverticulosis, since in this the related straining at stool likewise arises from stasis due to loss of dietary fibre; and E. coli conditions, like appendicitis and cholecystitis, should be particularly associated with diverticulitis, since in this work these latter are related to over-consumption, especially of sugar. It is, therefore, in the author’s opinion, of deep significance that in another series of 740 cases of diverticular disease, [22] brought forward to demonstrate a strong association with diabetes, the association of diabetes with the diverticulitis cases (22.8 per cent) was over double that with the diverticulosis cases (10.5 per cent). For later in this work it will, it is hoped, be shown that diabetes arises from the same over-consumption, especially of sugar, that has already been blamed here for the supervention of diverticulitis. III. Irritable Colon and Cancer of the ColonAs stated above in connexion with diverticulitis, there will be set out in Chapter IX the effect of over-consumption, arising from the refining of carbohydrates, on the bacterial population in the intestines — especially in the colon. In that chapter attention will be drawn to the evil-smelling nature of the stools of Westernized man, in marked and sustained contrast with those of any wild creature (but not in contrast with those of the domesticated dog or pig, often living quite substantially on our own refined carbohydrates). In that chapter the subject of intestinal toxaemia will be built up in outline from this simple basis. However, it is desirable to devote here a few words to the local effects of the toxic products discussed in that chapter. The author is confident that the non-specific diarrhoea, of considerable chronicity and unattended by any constipation, that not infrequently characterizes this condition, is due to the impact of these irritating putrefactive products on the wall of the gut. He is also confident, as the result of practical experience, that the successful treatment of this diarrhoea does not lie, as has recently been suggested by Harvey, Pomare, and Heaton, [23] in the giving of unprocessed bran, though a wholemeal loaf is always correct, but in the careful replacement of table sugar in all forms by raw and dried fruits and certain fresh vegetables, as set out in the diet card at the end of this work. Unless the offensive odour of these motions is attacked in this manner no real relief will in his experience be obtained. [24] He regards the direct action of unprocessed bran on the gut as invariably aperient. b. Cancer of the Colon In 1959, in the Journal of the New Health Society (Vol. XXXIV, No. 4, page 7) founded by the late Sir Arbuthnot Lane and now unfortunately in abeyance, the author wrote the following, to which he equally subscribes today: ‘The first of these local consequences is an intermittent putrefactive diarrhoea, and the chronic simple colitis to which, in the writer’s firm opinion, this may gravitate. But a graver local consequence is probably cancer of the colon. It is noteworthy that the frequency of cancer increases steadily in each successive part of the colon, cancer of the rectum being one of the commonest in the body. It is significant that the irritant action of any toxins on the intestinal wall must increase steadily in each of these successive parts, both on account of the actual greater production of toxins, and also on account of the progressive slowing that normally occurs, in the colonic contents as they pass onwards.’ He repeated this in 1960. [25] But an amendment is needed in that stasis, and the incidence of cancer, are both high in the case of the caecum. It is clear that any unnatural stasis must aggravate the above sequence, but as regards the actual irritants involved, the author believes that, although these have been blamed on the degradation of bile-salts, the labour of generations might be needed to establish which toxic products are mainly responsible for tumour formation — and yet that this labour would not achieve any greater practical prevention than is achieved by the foregoing reasoning plus the use of the nose, which will be alluded to in the later chapter. As one instance of the enormous difficulties that would be involved, the author has only to point to the problem of establishing in natural stools, let alone Westernized ones, the faecal microflora themselves, in which it has been stated by one authority, and quoted by several others, [26] that ‘whenever a man gets the idea that he is going to work out the bacteriology of the intestinal tract of any mammal, the time has come to have him quietly removed to some suitable institution’. What has been written above on cancer of the bowel is based on simplicity in reasoning and the presence of the unnatural feature just mentioned in the stools of Westernized man. The epidemiology has been set out convincingly by Walker [27] and by Burkitt [28] and shows how closely the condition follows the consumption of refined carbohydrates. IV. The Natural Treatment of Intestinal StasisAt first sight the natural treatment of intestinal stasis, that plays so big a part in the production of the condition just described, would appear to lie in taking all bread as wholemeal bread, and in taking all sugar as raw and dried fruit and as certain sweet vegetables such as beetroot, carrots, etc. This indeed is theoretically the most correct, and certainly the most pleasant, way of restoring to the diet the fibre that has been taken from it. But in practice serious obstacles at once present themselves. Quite apart from any trouble in getting hold of a true wholemeal bread, i.e. a brown bread that still contains all the natural bran (and some brown bread contains no bran at all), there is the question of expense. For to effect the above substitutions, at least as regards fruit, often requires more money than many people can afford to spend. Faced with this problem many years ago, when advising his naval patients and at times their families, the author began to experiment with himself in the taking of natural, unprocessed bran (that is, raw bran), as sold for a negligible sum at any corn chandler, at any seed shop, or even at any pet shop; or at a ‘health store’. He proceeded cautiously, but was soon widely prescribing this natural substance, and in 1941 wrote his first letter to the British Medical Journal, [29] describing 10 years’ experience with it and disposing of certain possible objections to its use. He was at that date the senior medical officer of the battleship King George V, and owing to the wartime scarcity of fruit and vegetables, especially at sea, found such bran invaluable for correcting constipation in the ship’s company. The ship’s canteen bought the bran by the hundredweight sack and sold it at the present equivalent of 1p per pound — which amount often lasted a man for several weeks. The bran was very popular with the sailors, as it enabled them to do without purgatives, and on one occasion, when the supply failed, many fell in at ‘Captain’s Request-Men’ to ask if it could be restored to them. Not only has the author used unprocessed bran in thousands of naval personnel at sea, but he has also used it for nearly 20 years during specialist duties as a physician in naval hospitals, where he always declined to use aperients, but relied instead on an enema if any serious arrest was already present and then solely on the unprocessed bran for future prevention. He wrote a second letter on this subject to the British Medical Journal in 1962 [30] and a third as recently as 1972. [31] He is glad to see that the use of this substance is at last spreading in the United Kingdom, but with at least 15 per cent of the population on habitual purgatives, as already stated, this spreading has a very, very long way to go yet. And of course the same applies to the substitution of a true wholemeal bread for white bread. It may be added that the author has by no means confined the prescribing of unprocessed bran to cases of simple constipation. He has used it in other saccharine manifestations, ranging from haemorrhoids to the diverticular disease described above; and as regards the latter, Mr. N. S. Painter has recently employed this treatment on a much larger scale, with most satisfactory results. [32] It is important to add that the taking of unprocessed bran should not be accompanied by the eating of any bread that is not truly wholemeal. It would be senseless to take such bran on the one hand, but exclude it from the bread on the other. Indeed, the author [31] has argued that, far from reducing the natural amount of bran incorporated in a true wholemeal loaf, as is so often done, it is usually much wiser to add 10 per cent of extra bran to the loaf, so as to help atone for some of the fibre lost in the refining of flour. In short a ‘110 per cent extraction’ flour is far better than a 90 per cent extraction flour. To this effect, some 5 years ago, the author succeeded in getting a ‘bran-plus’ loaf of this type introduced into the heart of London, where it is now being baked in increasing quantities (Messrs. Cranks, Marshall Street, London, W.1). The extra bran has proved no deterrent whatever to the demand for such bread, and the bran-plus loaf can also easily be baked in the home, by using the simple Grant method (Grant, Doris (1973), Your Daily Food. London: Faber & Faber). (Grant loaf recipe.) Finally, as regards the actual taking of unprocessed bran, although this substance has the advantages of cheapness and unimpaired vitamin content, the former being of decisive importance in hospital and other institutional use, there are a few precautions to be noted: a. There is a tendency to the production of flatulence for the first two or three weeks, until the gut becomes acclimatized, but this is an indication for a temporary reduction in the dosage, never for an abandonment of taking this most natural material. The author can understand that old or frail people require a longer and more gradual habituation, but this is rarely necessary in younger people — and was never necessary in the Navy. b. As regards the dosage, which is set out in the diet card at the end of the present book, this depends entirely on how much other fibre is taken in the diet. Wealthy people, who can afford plenty of fruit, will not need bran at all. But the poorer members of the community may need a great deal — anything from one tablespoonful morning and evening to one or two tablespoonfuls at meal times. c. The bran should be taken before meals, so as to prevent any indigestion from overloading of the stomach. The taking before meals also has the effect of reducing the calorie intake, as the bran itself has very few calories. This effect becomes valuable in cases of obesity. d. Unprocessed bran cannot be swallowed dry. It is best taken in a thick fluid — for example, a jug of pea soup can be made up and kept in a refrigerator: a little at a time mixed with the bran gives an easy and pleasant descent. Or the bran can be taken in porridge, Shredded Wheat, or other whole cereal, with milk. Or, of course, the bran can just be washed down in some water, as it usually was in the Navy. e. Finally, unprocessed bran is now being sold inside Cellophane wrappers. However aesthetically desirable this is, it is essential that those poorly off should realize that Cellophane wrappers are no more a necessity with bran than they are with, let us say, ordinary apples. The author has found that bran bought from any of the shops specified above is perfectly safe, as long as it is reasonably fresh from the mills and has been kept throughout under cover to protect it from mice, etc. Finally, constipation is especially liable to occur in old age, because the loss of teeth makes it difficult to bite up the coarse fruits and vegetables which supply the vital fibre. Thus, in one of the most beautiful, and certainly one of the most famous, pieces of English ever written, the 12th chapter of Ecclesiastes, the Bible tells us that in old people ‘the doors shall be shut in the streets, when the sound of the grinding is low’ (the grinders being the teeth). This trouble with the bowel rivals in importance the other troubles of old age so magically described in the above chapter, such as the frequency of passing water, due to the shrinking capacity of the bladder, which is rendered in the famous (but seldom appreciated) metaphor, ‘the grasshopper shall be a burden’ (i.e., the male organ of generation) — and there are few old men who would not agree with these dramatic words. (Incidentally the whole of the medical significance of the 12th chapter of Ecclesiastes was documented and set out in 1952 by 0. H. P. Pepper, [33] at that time Emeritus Professor of Medicine at the University of Pennsylvania in Philadelphia, to whom the author was indebted for valued personal communications on this subject.) However, to refer again to the constipation of old age, it must be repeated that though the unprocessed bran will supply the fibre here in a most practicable manner (and also the constituents of the vitamin-B complex often sadly deficient at this age), the bran needs to be introduced very gradually, because the preliminary flatulence, which is of little importance in younger people, can be very important indeed in older ones. Incorporation in a suitable vehicle to facilitate swallowing, as in (d ) above, is also essential in old people. As pointed out to me by Mr. Conrad Latto, Shakespeare in Coriolanus (Act I, Scene 1 speaking for the human belly, says, in brief, ‘I am the storehouse of the whole body, and what I receive I send through the blood to the heart, the brain and even the small inferior veins, and all I am left with for myself is the bran from the flour’. It is feared that in Westernized countries today this latter is far from being the case, the belly usually being left with no bran at all, and as a consequence the serious maladies set out above are needlessly incurred. It is hoped that what has been written may help to correct this state of affairs, and meanwhile we pass on to a study of these same inferior veins. References1. Cleave, T. L., and Campbell, G. D. (1968), Brit. Med. J., 1, 579. 2. Campbell, G. D., and Cleave, T. L. (1968), Ibid., 3, 741. 3. Manousos, O. N., Truelove, S. C., and Lumsden, K. (1967), Ibid., 3, 760. 4. Burkitt, D. P., Walker, A. R. P., and Painter, N. S. (1972), Lancet, 2, 1408. 5. Morris, J. N. (1941), Ibid., 1, 5 1. 6. Connell, A. M., Hilton, C., Irvine, G., Lennard-Jones, J. E., and Misiewicz, J. J. (1965), Brit. Med. J., 4, 1095. 7. Lancet (1964), 2, 631. 8. Wells, C. (1949), Brit. J. Radiol., 22, 449. 9. Carlson, A. J., and Hoelzel, F. (1949), Gastroenterology, 12, 108. 10. Spriggs, E. I., and Marxer, O. A. (1925), Quart. J. Med., 3, 1. 11. Lewis, J. H. (1942), The Biology of the Negro. Chicago: University of Chicago Press. 12. Painter, N. S., and Burkitt, D. P. (1971), Brit. Med. J., 2, 450. 13. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 42, No. 2, 55. 14. — and Campbell, G. D. (1966), Diabetes, Coronary Thrombosis, and the Saccharine Disease, 1st ed. Bristol: Wright. 15. Painter, N. S. (1967), Brit. Med. J., 3, 434. 16. Cleave, T. L., Campbell, G. D., and Painter, N. S. (1969), Diabetes, Coronary Thrombosis, and the Saccharine Disease, 2nd ed. Bristol: Wright. 17. Painter, N. S. (1964), Ann. R. Coll. Surg., 34, 98. 18. — and Truelove, S. C.(1964), Gut, 5, 201. 19. Kaye, M. D., and Kern, F. (1971), Lancet, 1, 1228. 20. Parks, T. G. (1969), Brit. Med. J., 4, 639. 21. Latto, C., Wilkinson, R. W., and Gilmore, O. J. A. (1973), Lancet, 1, 1089. 22. Schowengerdt, C. G., and Hedges, G. R. (1969), Arch. Surg., 98, 500. 23. Harvey, R. F., Pomare, E. W., and Heaton, K. W. (1973), Lancet, 1, 278. 24. Cleave, T. L. (1973), Ibid., 1, 1443. 25. — (1960), On the Causation of Varicose Veins, 35. Bristol: Wright. 26. Gorbach, S. L., Laila Nahas, Lerner, P. I., and Weinstein, L. (1967), Gastroenterology, 53, 845. 27. Walker, A. R. P. (1971), S. Afr. Med. J., 45, 377. 28. Burkitt, D. P. (1971), Cancer, 28, 3. 29. Cleave, T. L. (1941), Brit. Med. J., 1, 461. 30. — (1962), Ibid., 1, 191. 31. — (1972), Ibid., 2, 409. 32. Painter, N. S., Almeida, A. Z., and Colebourne, K. W. (1972), Ibid., 2, 137. 33. Pepper, O. H. P. (1952), Am. J. Med. Sci., 223, 589. Chapter IVVaricose Veins, Deep Venous Thrombosis, Varicocele, and HaemorrhoidsVARICOSE veins, deep venous thrombosis, varicocele, and haemorrhoids are held here normally to be unequivocal manifestations of the saccharine disease, and also to exemplify in striking manner the value of the approach set out in Chapter I — embracing the law of adaptation, and the distinction between, on the one hand, bodily defect and, on the other hand, personal make-up reacting with a new environmental factor. This contention was first put forward in 1950 [1] and later amplified in 1959 [2] and 1960, [3] and will now be summarized here. I. Varicose Veins
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


 Fig. 3. — The relationship of the colon to the arteries (cross-hatched) and veins (black) at the back of the abdomen (diagrammatic only). [3] (From an original drawing by Surgeon Commander R. Y. W. Lambert R.N.) |
For, it must be added, it is not only the iliac colon that is related to the external iliac vein; on the right side the caecum is adjacent to the right external iliac vein, and if the caecum becomes distended as the result of colonic stases, it does not tend to rise upwards towards the liver but to fall downwards towards the pelvis, and so may cause a similar obstruction in the right vein. Indeed a prolapsed caecum is quite common, as surgeons who operate in this region know well.
It must be emphasized that there is no question of these parts of the colon floating freely in the abdomen, which would virtually preclude any local pressure on the external iliac veins. They have no mesentery (unless the caecum is prolapsed over the vein into the pelvis, when the question of a mesentery becomes relatively unimportant), but are in direct contact with the (external iliac) veins. Indeed R. J. Last, [13] in his work on anatomy (1966), describes the descending colon as ‘plastered down’ by the peritoneum. Moreover, the commencing pelvic meso-colon, which follows the line of the external iliac vein, but in an upward direction, is at first so short that the beginning of the pelvic colon is also closely applied to the vein. It may also be important that a loaded pelvic colon lower down could lead to a pulling across the vein, either by its direct continuity with the iliac colon or by its mesentery, [14] just described; indeed some may prefer this alternative view. It must always be remembered that the resting pressure of blood in the iliac vein is only a few millimetres of mercury. For this same reason the intervention of the external iliac artery, in which the pressure of blood is vastly higher, would offer no protection, as any colonic pressure would be at once transmitted through it to the vein.
2. Significance of Preponderances in the Left Leg
To look more closely into this question of the relative incidence of varicose veins on the two sides of the body, it is clear that in the erect position, since the iliac veins are running almost vertically downwards, any positional superiority of the left colon over the caecum, in being able to obstruct the vein, will be small, but that in the supine position, since the left colon will still be crossing over the vein, whereas the caecum on the right may be falling away from the vein, laterally, this superiority of the left colon will become considerably magnified. It is consistent with these facts that the incidence of varicose veins is only about 10 per cent greater on the left side, [15] whereas the clinical incidence of ileofemoral thrombosis, in many references, is nearly three times greater on the left side, as shown in
According to Various Observers |
|||||
| Date | Author |
Total Cases
|
Percentage
Incidence on Left |
Percentage Incidence
on Right |
Bilateral
|
| 1784 | White [16] | 9 | 65 | 35 | |
| 1938 | Atkins [17] | 34 | 82 | 9 | 9 |
| 1940 | Barker [18] | 210 | 72 | 28 | |
| 1943 | Ehrich and Krumbhaar [19] | 16 | 50 | 18.7 | 31.3 |
| 1967 | Negus [20] | 88 | 53.5 | 27 | 19.5 |
| 1967 | Cockett, Lea, Thomas and Negus [21] | 57 | 70 | 30 | |
| 1967 | Mavor and Galloway [22] | 38 | 75.3 | 24.7 | |
For varicose veins occur chiefly in people who are up and about for most of the day, though they are recumbent at night. But ileofemoral thrombosis occurs predominantly in bed-patients, whether due to illness, childbirth (‘white leg’), or following operation, the patient thus being nearly always in the supine position.
The significance of the figures in Table II is not lessened by the fact that fibrinogen and other tests often show thrombosis to be present on both sides. For quite apart from thrombosis beginning during the trauma of certain (especially pelvic) operations, to be mentioned later, Doran and others [23] have shown that during any major operation the venous return is always slowed by a half, and not infrequently slowed to the level found in a paralysed limb, so no doubt nuclei of thrombosis often do form on both sides (for Virchow showed long ago how important slowing is in the causation of thrombosis). But whether these nuclei increase in number, expand, and coalesce until the state of clinical thrombosis is reached, often around the tenth day and with or without pulmonary embolism, depends on an added factor, which the present author believes to be the unnatural loading of the colon, described above. Therefore, to him the clinical thrombosis is what is of paramount importance, and it is the great preponderance of this clinical thrombosis on the left side that is so revealing and that points to the prophylaxis shortly to be advanced. On this line of reasoning fibrinogen-testing soon after operation, recently described as largely impracticable [24] in any case, seems often to be irrelevant.
(It must be added parenthetically at this juncture that very similar reasoning to the foregoing can explain the causation of varicocele, which in the vast majority of cases is confined to the left side, since on this side the iliac colon crosses directly over the left spermatic vein, whereas on the right side the caecum does not cross over the right spermatic vein, and in addition is partly kept away from it by the larger mass of the external iliac vessels.)
As regards the argument sometimes heard, that with an unrefined diet the extra bulk of the colonic contents would lead to greater, not smaller, pressures on the iliac veins, the following considerations must be borne in mind, as the author has set out elsewhere. [25]
- The complex hydrodynamic factors within the abdominal walls would preclude this being the case, however voluminous the colonic contents, unless the specific gravity of these contents were sufficiently raised above that of the peritoneal fluid, which, for evolutionary reasons, would be unlikely to occur except in the presence of unnatural stasis (and consequent accumulation of intestinal sand, which forms a considerable proportion of these contents). And it is to be noted that the behaviour of a stool in water is an unreliable guide in this respect, because any trapped gases of intestinal fermentation in the stool could lead to its floating when otherwise it would sink.
- The extra bulk arising from the diet is held here to be more than compensated by the much faster transit time. In this respect the author is privileged to quote the following personal communication (dated 10 September, 1972) from Mr. Anthony Barker, who has provided much vital information on this subject from Africans living tribally, as seen above and elsewhere in this work.’… The Zulus do have more frequent and more bulky stools than do the whites of England, but the crucial point is that their transit times are much more rapid, averaging only 24 to 36 hours. In answer to your question about findings at operation, a loaded colon is quite exceptional in these people.’
- Finally, there is the actual sensation of colonic well-being so familiar to people having a natural consumption of fibre and consequently a fast intestinal transit time. To suggest to those who clearly recognize this definite sensation that it is based on colonic loading, instead of colonic emptiness, would be met with astonishment; and palpation of the abdomen would rapidly settle the matter.
3. The Rising Incidence of Pulmonary Embolism and Deep Venous Thrombosis in the Legs
It is vital to the argument now being presented that the incidence of pulmonary embolism, most of which is due to deep-leg thrombosis, has been rising very markedly in this country in recent years. A crucial paper by Morrell, Truelove, and Barr, [26] working in the Radcliffe Infirmary and Churchill Hospital, Oxford, shows that the incidence of this condition increased approximately fivefold in the decade 1952-61, and that though about a third of these cases were postoperative, the remainder were medical bed-patients, who had had no operation at all (thus suggesting that what is concerned in this rise may be something quite independent of an operation itself). These authors also quote European studies showing results not inconsistent with their own, with the frequency of pulmonary embolism and leg thrombosis decreasing during, and immediately after, each World War, but always recovering later, to resume a steady upward trend.
This rising incidence of pulmonary embolism and leg thrombosis is perfectly in accord with the general causation put forward here — the ever-increasing consumption of refined carbohydrates in Westernized countries, which has culminated in present transit times of the bowel contents now being about twice as long as the natural transit times (see Chapter III). But what is so instructive is that during the period now under consideration there has been a special aggravation of this cause, which will now be set out and which will be seen greatly to strengthen the whole of the present argument. Perhaps slightly because of the shortage of nurses and the shortening of their hours of work, this aggravation has consisted in the shading off, or even open abandonment, some 20 years ago, of various hospital preoperative purgative and enema routines, except for special operations, as on the bowel. It was Mr. Conrad Latto who first spoke to the author of this change in surgical practice during the 1950’s, which came in gradually and to varying extents in different localities, and the same thing was confirmed by the late Mr. A. Elliot-Smith (of the Radcliffe Infirmary), Mr. L. Knights, and others, including Surgeon Vice-Admiral J. Watt, who consulted senior naval nursing staff on this point. There seems no doubt that this change has commonly occurred during the 1950’s, and its possible relevance (on the argument at present being advanced) to the big increase in pulmonary embolism and leg thrombosis over much the same period, described above, is obvious. It is to be noted, too, that the frequent substitution of suppositories for enemas, which seems to be another labour-saving change of the same type that has taken place, would also have an unfavourable effect with regard to the removal of any high accumulations, such as those present in the vital iliac colon, and even higher.
And now, with regard to the realities of the colonic stasis at present being discussed, the author would like to make two quotations. The first is taken from Mr. Harold Dodd’s foreword to the author’s early monograph on varicose veins, now largely superseded by the present volume: ‘It is my practice to teach that patients confined to bed seldom empty the colon; even if they have a daily action, it is merely an overflow. I have been impressed with this again and again when operating … their bowels are often laden with plastic faeces from the caecum to the rectum.’ Loading of the iliac and lower colon is of course well recognized, as inquiries of many surgeons have confirmed, and the author would add that he has, himself, on countless occasions rolled a loaded iliac colon under the hand on ordinary clinical palpation of the abdomen, as other physicians will remember doing, too.
The second quotation is from a much less distinguished source, but, considering the seriousness of the present situation over leg thrombosis, the author thinks that such a clear and absolutely disinterested observation is well worth reproduction, and that where the truth is so pressing,
‘One glimpse of it within the Tavern caught,
Better than in the Temple lost outright.’
Thus I refer to Dr. John Rowan Wilson’s (nom de plume for the late Dr. John Robinson Wilson) contribution to the medical columns of The Spectator on 24 August, 1970:
‘A friend of mine recently went into hospital for the treatment of depression. She had been admitted for the same condition a number of years ago, and she was fascinated to see how everything had changed. In the old days the emphasis was all on spit and polish and the traditional nursing routine. Patients were awakened at six o’clock in the morning, beds had to be neat and tidy, temperature and pulse were religiously charted. Sister was obsessive about bowel movements: if anyone missed a day it was big news; aperients and enemas were immediately enlisted to bring her up to scratch.
‘After a ten years’ interval the atmosphere was unrecognizable. It was cheerful, chatty and informal. The emphasis was not on physical treatment but on making the patient feel at home and allowing her some freedom to express herself. The nurses were far more interested in home backgrounds and troubles with husbands and children than with temperature charts and bowel movements. Most important of all, patients were encouraged to form a mutually supportive community. They spent most of their time talking to each other. “And what did they talk about?” I asked my friend. “Their bowels, mostly”, she said. “They were all as constipated as hell.” ‘
4. Straining at Stool not considered here the Key Factor
Apart from the special instance of haemorrhoids (where a particular muscle-factor is involved, as shown in Fig. 4), the author, himself, cannot accept, what has several times been suggested to him, that straining at stool is of any great significance in the aetiology of varicose veins or deep venous thrombosis. For one thing, if straining were aetiologically important, venous ills would be expected to be prominent in patients with chronic cough, which is definitely not the case. Furthermore, it is quite unnecessary to postulate any such high venous pressures in the aetiology. What is much more deadly than a temporary high pressure, that is to some extent natural and adapted to, is a long-continued low pressure that is not natural and not adapted to. Thus a series of long jumps, or a cross-country run, inflicts enormous strain on the spring ligament supporting the arch of the foot, but normally leaves it unscathed, whereas the unnatural constant strain of even a stone of overweight can flatten it right out. This ‘inevitability of gradualness’ is also seen in the case of the tiny but long-continued forces of the starfish eventually breaking down the vastly greater but less sustained forces of the oyster, which is thus opened and devoured. It is not wise to minimize the unnatural and continual back-pressure effect on the valves of a vein, that must result from a loaded colon lying across the vein, which back-pressure the valves are not evolved to support, and due to which they tend to dilate and become incompetent.
Stemming from the above it has even been suggested that the squatting position at stool, by reducing the effects of straining, explains the lack of venous ills in tribal Africans, referred to earlier. But anyone who tries an unrefined diet knows that with such a diet the call to stool is so urgent that no straining worth discussion is possible in any case, but that, per contra, with a refined diet the straining can be very severe no matter what position is adopted. All this quite apart from the fact that some crouching is instinctively adopted, anyway, even at the height which has been found most convenient for the construction of closet seats. What is needed in Westernized countries today is not the reconstruction of millions of these seats, but the restoration to the diet of the fibre of which it has been robbed.
 Fig. 4. — A, Superior haemorrhoidal vein compressed between the contracted sphincter and a hard faecal mass. B, Superior haemorrhoidal artery unaffected by compression and continuing to supply blood to the venous plexus. (Reproduced with permission of the publisher from A. G. Parks.) [35] |
With further regard to straining at stool, it has been postulated that past straining, through having damaged the venous valves, is the essential cause of postoperative thrombosis. Quite apart from the failure of this postulate to explain the striking clinical preponderance on the left side, already alluded to, a strong additional reason can be advanced against it. For if past straining were the essential cause, then any operation cases with varicose veins (themselves constituting the best evidence of past damage to the valves) would be expected to suffer from postoperative thrombosis decidedly more often than operation cases without varicose veins. Yet Kemble [27] has recently shown in a survey of 280 cases at the Middlesex Hospital that there was no difference in postoperative thrombosis between the two groups. The fact is that in the supine position, where the blood is flowing horizontally, the valves in the veins are hardly being used at all and so their integrity is relatively unimportant (which is, of course, why varicose ulcers heal up in this position). But be it noted that, in sharp contrast to the above, the result of this Middlesex survey is in no way harmful to the view that the causation of most postoperative thrombosis lies in unnatural colonic loading, for such pressures will slow the blood flow in the external iliac veins, whatever the state of the valves below.
There must also be considered the question of varicose veins in pregnancy. It is established that these normally appear early in pregnancy, when the fetus is too small to be able to exert any pressure on the veins. (This, quite apart from the fact that evolution must have ensured that no such pressure shall occur anyway.) Now it is well known that a severe constipation is likely to occur early in pregnancy, precipitated by the common occurrence of morning vomiting at this time, which interferes with the food intake. It is thus easy to relate the varicose veins to the pressure of a loaded colon but not to straining at stool, for they usually disappear after the pregnancy is over, which any stretched valves of the veins would not allow (the valves being fibrous in structure).
It is also important to add to the foregoing that the attribution of venous ills to straining at stool, instead of to direct colonic pressure on the iliac veins, would be a very serious thing as regards therapeutics. For postoperative leg thrombosis often cannot be due to present straining at stool since the thrombosis often happens before any such straining is possible. So prophylaxis would often be impossible, too. Whereas, if direct colonic pressure is the cause, prophylactic attention to the state of the bowel, as will shortly be described, becomes not only of crucial importance but also perfectly feasible.
5. The Question of an ‘Iliac Compression Syndrome’
We must now pause to examine other theories of causation of the venous ills we have been discussing. To explain the big difference in the incidence of femoral thrombosis on the two sides Aschoff [28] and others, who regard recumbency as the dominant cause of most femoral thrombosis, have contended that the reason lies in the right common iliac artery crossing over the left common iliac vein, and Williams [29] has even implicated this normal anatomical relationship in the production of varicose veins themselves. Meanwhile, to explain the even bigger difference in the incidence of varicocele on the two sides, most textbooks of surgery give the fact that the left spermatic vein opens into the left renal vein at right-angles, without a valve, whereas the right spermatic vein opens into the vena cava obliquely, with a valve. But both the above explanations are completely incompatible with the law of adaptation, as set out in Chapter I, and furthermore each of the explanations is rendered weaker by the existence of the other. For it would be a coincidence indeed if evolutionary errors occurred in both the right iliac artery and the left spermatic vein. In that case the body would be expected to be full of errors, whereas the figures for hereditary defects in Chapter I show just how rare evolutionary errors are — and moreover they are not errors in mechanical conception.
In connexion with the foregoing, we must take note of a more recent elaboration of the first of these postulated anatomical causes. F. Cockett and others, also seizing on the marked preponderance of ileofemoral thrombosis on the left side, likewise incriminate the right common iliac artery crossing the left common iliac vein ‘as the main aetiological factor’ in the production of the thrombosis, and have advanced radiological and post-mortem findings in support of such a mechanism, under the title of ‘The Iliac Compression Syndrome’. [30]
For those, however, who steadfastly refuse to blame the evolutionary adaptation of the human body, but who look instead for an unnatural factor in the environment, as the cause of the present troubles, this view presents no terrors. In the first place the phlebograms, and the denting of, and adhesions inside, the vein opposite the crossing, which these writers have found in 14 out of 100 cadavers, do not include any comparable studies in populations who do not suffer from these venous ills, such as the tribal Africans mentioned above. If the findings in these subjects proved to be much the same as in Westernized ones, such findings would emerge as not of pathological significance. But if such findings were absent, there is an explanation for their presence in Westernized subjects, which is not in conflict with human evolution. This is that in Westernized subjects, in whom these venous ills abound, the crossing of an unnaturally loaded colon over the lower iliac vein, through interfering, however slightly, over many years with the venous pressures in the vein above this crossing, leads to the very effects of the artery on the vein which the writers describe.
Meanwhile, in order to explain the cases of deep thrombosis in the right leg, which in the present book is related to stasis in the caecum, the above writers incriminate yet another artery — the right external iliac artery pressing on the right external iliac vein. Lastly, the compression syndrome cannot explain the very big preponderance of varicocele on the left side, which a colonic cause can do.
In the second place, the ‘iliac compression syndrome’ cannot explain the great increase in deep leg thrombosis that has occurred over the past 20 years, as has already been set out here.
Finally, there is a third and subtler consideration that can be advanced against this syndrome, which may be expressed as follows: if the left hand encircles with moderate pressure the right wrist, and if the right hand is then (a) hung downwards and (b) repeatedly clenched, it is obvious that the veins of the hand will at once become prominent. Similarly, any arterial compression effect on the left iliac vein, as described in the above syndrome, would become far more noticeable when the subject was erect and at exercise than when he was lying down and at rest. Therefore varicose veins, which are commonly seen in people who are up and about, would be expected to have a much greater left-sided preponderance than would deep leg thrombosis, which is so often associated with recumbency. Yet in reality the exact opposite occurs (which, however, accords perfectly with a colonic cause, as already shown).
That the above anatomical sites, and Poupart’s ligament too, form natural areas of arrest in cases of spreading thrombosis is not contested for a moment, but this leaves the reason why the thromboses occur in the first place unsolved, and the crucial difference between the above postulate and the one advanced here is that the latter leads to vital possibilities in prevention. For if the natural artery-pressure were basically implicated in the causation of deep leg thrombosis, such pressure could not normally be removed and so no prevention could be undertaken. But if a colon, unnaturally loaded through the diet of Western civilization, is basically implicated, prevention becomes immediately possible. This would consist ideally in restoring the natural fibre to the diet by taking substances such as the unprocessed bran described in Chapter III, so that the natural transit time of approximately 1-1/2 days (Chapter III) replaced the present 3-5 days seen in Westernized societies. If this restoration were not feasible, suitable bland aperients would be needed, with or without enemas as necessary. Such steps would be important in medical bed-patients, and also in confinement and operation cases (where the restoration of the natural transit time, if possible before the event, would in the opinion of the present writer bring about a rapid reversal in the climbing incidence of leg thrombosis). There would in these latter cases then be no need for the present extremely early getting-up after operation, which, as in the case of leg exercises, has signally failed to prevent the quadrupling of the incidence already referred to. It is, however, fully realized that a considerable number of thromboses are due to inevitable direct trauma to the iliac veins in certain (especially pelvic) operations, which cases may obviously need further measures, such as heparin, etc.
It is also clear, from the cause advanced here, that, as regards deep thrombosis, a prone position of the patient is far safer than a supine one, since in the former position no colonic accumulations can press on the (iliac) veins in any case, and indeed it is fair to point out that the very fact that this position has been found so beneficial [31] in practice is itself in favour of the correctness of this cause.
Finally, as regards the frequent earlier implication of the deep calf veins than the iliac and femoral veins in the thrombotic process, there is no reason why the repository of the back-pressures described above should not first be more evident in the more peripheral veins than in the more central ones.
Further to all the above, it has been recently demonstrated [32, 33] that increasing the blood-flow in the lower limbs during operation, by intermittent compression with inflatable splints, is ‘a potent prophylactic against postoperative deep vein thrombosis’. This evidence dovetails perfectly with the prophylactic step advanced here, of preventing any impediment to the blood-flow from pressure on the veins by a loaded colon.
6. Prophylaxis of Deep Venous Thrombosis
Amongst those who have put whole surgical wards on to unprocessed bran, in an effort to reduce the incidence of postoperative thrombosis, on the argument just set out, are Mr. Conrad Latto of the Royal Berkshire Hospital, Reading, and Surgeon-Commander N. J. Blacklock of the Royal Naval Hospital, Haslar. Both have been immeasurably helped by the complete conviction, and from this the complete co-operation, of the sister in charge of the ward, which, in the author’s experience, is without question the most important factor of all in success. Mr. Latto [34] has already reported excellent results with these patients as regards the behaviour of the bowel, resulting in the elimination of aperients from the ward, and Surgeon-Commander Blacklock has confirmed this finding in a personal communication to the author. As regards the occurrence of postoperative thrombosis, it is clear that single-ward experience can never become more than a pointer, encouraging others to carry out a comprehensive trial. With this absolute proviso, Mr. Latto writes (March, 1973): ‘We have had no case of postoperative thrombosis in this ward for over 18 months. One case of thrombosis was admitted from outside and had a fatal embolism — and it may be added that at post mortem the left colon was solid with hardened faeces.’ Surgeon-Commander Blacklock’s experience to date is similar in that ‘We have had only one case of postoperative thrombosis in a little over one year, and this occurred in a man who had established congestive cardiac failure, which was presumed to be the basic cause in this case.’ Eight months later (November, 1973) these favourable results continue, and recently Mr. Maurice Frohn has introduced the taking of unprocessed bran into his surgical wards at the Bethnal Green Hospital, London, in an effort to prevent postoperative thrombosis. The author is confident that Mr. Frohn will have much to contribute to this form of prophylaxis, especially in gastro-intestinal operations.
Finally, it must once again be emphasized how much everything depends on the co-operation of the ward sister. Thus, Mr. Latto’s patients are given three tablespoonfuls of bran and are allowed to get it down as they please during the day — in milk, soup, water, etc. In Surgeon-Commander Blacklock’s patients the bran is taken along with the meals, or mixed in with tomato juice, in which it has been found most palatable and easy to take. It is the ward sister who will ensure that operation cases have no accumulations in the rectum, either by the taking of the bran or, if there has not yet been time for this to work, by clearance enemas.
7. Haemorrhoids
With regard to haemorrhoids, their causation is held here to be due to a very similar mechanism to that involved in the production of varicose veins and varicocele, the only difference being that in this case the pressure of faecal accumulation is exerted on veins within the bowel instead of on veins without. This pressure effect is greatly aggravated by straining at stool, in the effort to pass the constipated motion (see Fig. 4). It must be added that constipation as an important factor in the causation of haemorrhoids has long been recognized.
8. Further Considerations
As regards another condition mentioned earlier, an added note may be made on the tendency for varicocele to become much less conspicuous as age advances. In the author’s opinion this may lie in young people, as they grow older, getting tired of the waste of time and effort caused by constipation and gradually joining the army of 7 million regular aperient-takers in this country, already referred to in the last chapter.
It is also worth pointing out that, in the absence of obvious pressure causes, such as tumours, or cirrhosis of the liver, no clinical varicosities occur in the human body except where obstruction due to colonic stasis can account for them. Indeed, this peculiar localized distribution of clinical varicosities in the body weighs heavily against any postulated general cause of such varicosities — such as, for example, some blood condition. And for this reason any attack on postoperative thrombosis by injections of heparin, etc., however expedient this may appear, must — as long as a basic cause is not removed — always savour of two wrongs not making a right. This at least is the opinion of the present writer, holding the view on the causation that he does.
* * *
To turn back, it now becomes possible to see very clearly why there is so great a difference in the incidence of all these venous obstructions in the two groups of Negroes which were referred to. For the Negroes in the United States are eating the same refined carbohydrates as are the whites, whereas those living tribally in Africa are subsisting on a diet almost wholly composed of crudely ground maize or other unrefined carbohydrates. The very large quantity of fibre ingested by the tribal Africans has a striking effect on the quantity and the quality of the stools. These are passed twice a day and are extended like a ribbon of toothpaste some 15 in. long, and of the diameter of the middle finger. They are in fact known locally as the ‘toothpaste stool’.
In this connexion it is important to point out that the rate of passage of the colonic contents cannot be assessed by the regularity of the motions passed. These may be passed with the utmost regularity — but may always be one day late! The rate of passage can, in fact, only be assessed by the consistency and diameter of the motion. If the rate is the natural one, i.e., if there is no unnatural stasis present, the consistency will always be soft and the diameter not appreciably greater than that of the middle finger.
The reality of colonic stasis in Westernized countries is revealed by the enormous consumption of aperients in these countries, as shown by the M. R.C. research workers’ figures set out in Chapter III. The reality of the stasis is likewise revealed by the dramatic change in the rate of passage of the colonic contents produced by restoring to the diet the fibre removed in the refining of flour, as in the taking of unprocessed bran described in the diet card at the end of this volume and referred to in Chapter III.
III. Personal Build and Heredity, in the Production of Varicose Veins
There are few more pronounced examples in the body, of differences in personal build, than occur in the human colon, which varies greatly, not only in its general position, but also in the length of its mesenteries. Consequently there is great scope in some colons, when unnaturally loaded, for pressing on the iliac veins, whereas in others there is no scope at all. Therefore, on a diet containing refined carbohydrates some persons will develop varicose veins and some will not. But, let it be noted, on a diet of unrefined carbohydrates, with no colonic stasis, no persons will develop varicose veins, no matter what the build of their colons.
Exactly the same type of argument applies to the occurrence, in the presence of a refined diet, of varicocele in some persons but not in others. And likewise to the occurrence of haemorrhoids. As regards haemorrhoids, it has been known for a very long time that colonic stasis in some persons is centred in the rectum itself. In fact over 30 years ago Arthur Hurst introduced the term ‘dyschezia’ for just this form of constipation. It is therefore easy to understand why, though these venous conditions (e.g., varicose veins and haemorrhoids) do have a tendency to occur together, they very frequently occur separately.
* * *
Finally, it will now be seen that, against the above background, the question of heredity is of no practical importance, because, as stated in Chapter I, it is just as easy to inherit personal build as bodily defect. Therefore, the presence of any hereditary element in varicose veins, varicocele, or haemorrhoids does not alter the fundamental situation one iota, nor our approach to it as regards treatment. Any preoccupation with heredity, in fact, would, as stated in the earlier chapter, be a case of drawing a red herring across the trail.
IV. The New Indications in the Prevention and Arrest of Varicose Veins, Varicocele, and Haemorrhoids
The author would be the first to agree that the evolutionary and racial evidence for the view advanced here, on the causation of these venous conditions, needs the added support of direct experimental studies, involving barium meals and other devices; and indeed it is his ambition to initiate such studies in the future. He would like, for example, to see what proportion of people with well-marked varicose veins in the right leg, or with a right varicose ulcer, have a prolapsed caecum, compared with people without these conditions. Such cases as Mr. Conrad Latto and other friends have looked into for the author, via barium meals, have for the most part shown partial or complete prolapse of the caecum, though even a normally placed caecum, if distended, could edge over onto the external iliac vein. Very recently a complete absence of gravitational ulcer has been reported in 9000 Iranian patients examined in Iran [36] — and their food was unrefined wheat and unrefined barley. Clearly all this points to a hopeful approach in treatment for the unfortunate sufferers from leg ulcer.
Believing as the author does, then, in the view advanced here, and unless experimental studies destroy it, he considers the essential step to be taken in all these venous conditions is the same substitution of unrefined carbohydrates for the refined ones — that is to say, basically, the substitution of raw and dried fruits for sugar, and sweetstuffs, etc., that contain sugar; and of a true wholemeal bread for white bread and all confectionery, etc., containing white flour. But no other dietetic steps are needed, and no harsh régime is therefore in question.
The above dietetic substitution will itself have a profound effect on the action of the colon, but if the stools do not change adequately to the natural form described above, the process can easily be completed by the taking of a little unprocessed bran each day, as set out in the card mentioned.
The above steps effectively remove the cause of all three of the venous conditions now under consideration. This may be sufficient treatment of itself in the early stages of the conditions, but of course local treatment will obviously be indicated, also, in the later stages — just as the same diet will prevent and arrest dental disease, but will not save a tooth from needing local treatment once a certain stage in the disease-process has been reached.
Local treatment, however, must never displace the removal of the cause. This is well seen in the case of postoperative femoral thrombosis and pulmonary embolism, the incidence of which, in spite of all the leg exercises, breathing exercises, and early ambulations, has, as already stated, nearly quadrupled in recent years. No one who understands the argument set out here, and who gives a glance at the foods eaten in the ordinary hospital, will share in the general perplexity occasioned by this increase.
Furthermore, quite apart from the question of persistence and recurrence, one of the decisive advantages in the conception of a single saccharine disease is the futility revealed of trying to ‘get away with’ the surgical treatment of one of the manifestations of the disease without simultaneous permanent removal of the cause, by the dietetic steps indicated above. For unless this removal of the cause is instituted, the patient remains completely exposed to one of the other manifestations. For example, where is the profit in having, per se, a haemorrhoid injected, if later all the teeth are to be lost from pyorrhoea? Better to keep the haemorrhoid, if it forces a dietetic reform. Otherwise, it is submitted that this would be another case of trying to be clever at Nature’s expense.
References
1. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 42, No. 2, 550.
2. — (1959), Lancet, 2, 172.
3. — (1960), On the Causation of Varicose Veins. Bristol: Wright. (U.S.A.: Williams & Wilkins Co., Baltimore.)
4. Foote, R. R. (1952), Varicose Veins, 2nd ed., 38. London: Butterworths.
5. Menendez, C. (1960), personal communication quoted in reference 3.
6. Kozoll, D. (1963), personal communication, quoted in Cleave, T. L., and Campbell, G. D. (1966), Diabetes, Coronary Thrombosis, and the Saccharine Disease, 1st ed. Bristol: Wright.
7. Lewis, J. H. (1942), The Biology of the Negro. Chicago: University Press of Chicago.
8. Dodd, H. (1964), Lancet, 2, 809.
9. Barker, A. (1964), Lancet., 2, 970.
10. Burkitt, D. P. (1972), Brit. Med. J., 2, 556.
11. Cleave, T. L. (1972), Ibid., 3, 177.
12. Brash, J. C. (1948), Cunningham’s Manual of Practical Anatomy, 11th ed., 2309. London: Oxford University Press.
13. Last, R. J. (1966), Anatomy, Regional and Applied, 4th ed., 401. London: Churchill.
14. Cunningham’s Manual of Practical Anatomy (1937), 9th ed., 325. London: Churchill.
15. Weddell, J. M. (1969), Brit. J. Prev. Soc. Med., 23, 179.
16. White, C. (1784), quoted in Negus, D. (1970), Ann. R. Coll. Surg. Engl., 47, 92.
17. Atkins, H. J. B. (1938), Guy’s Hospital Reports, 18, 92.
18. Barker, N. W., Nygaard, K. K., Walters, W., and Priestley, J. T. (1940), Mayo Clin. Prac., 16, 33,
19. Ehrich, W. E., and Krumbhaar, E. B. (1943), Amer. Heart J., 26, 737.
20. Negus, D. (1970), Ann. R. Coll. Surg. Engl., 47, 92
21. Cockett, F. B., Lea Thomas, M., and Negus, D. (1967), Brit. Med. J., 2, 114.
22. Mavor, G. E., and Galloway, J. M. D. (1967), Brit. J. Surg., 54, 1019.
23. Doran, F. S. A., Drury, M., and Sivyer, A. (1964), Ibid., 51, 486.
24. — (1973), Brit. Med. J., 2, 612.
25. Cleave, T. L. (1972), Ibid., 4, 612.
26. Morrell, M. T., Truelove, S. C., and Barr, A. (1963), Ibid., 4, 830.
27. Kemble, J. V. H. (1971), Brit. J. of Hosp. Medicine, 6, No. 6, 726.
28. Aschoff, L. (1924), Lectures on Pathology, 253. New York: Paul B. Hoeber.
29. Williams, T. H. (1959), Lancet, 1, 1010.
30. Cockett, F. B., Lea Thomas, M., and Negus, D. (1967), Brit. Med. J., 2, 14.
31. Osborn, D. M., and Osborn, G. R. (1965), Lancet, 1, 983.
32. Sabri, S., Roberts, V. C., and Cotton, L. T. (1971), Brit. Med. J., 4, 394.
33. Hills, N. H., Pflug, J. J., Jeyasingh, K., Boardman, L., and Calnan, J. S. (1972), Ibid., 1, 131.
34. Latto, C. (1972), Ibid., 3, 705.
35. Parks, A. G. (1956), Brit. J. Surg., 43, 337.
36. Griffiths, W. A. D. (1972), Brit. Med. J., 2, 770.
Chapter V
Dental Caries: Periodontal Disease
IT is not proposed to go deeply into the evidence linking dental caries, and to a large extent periodontal disease, with the consumption of refined carbohydrates, since this is already widely recognized. The author will therefore confine himself to the most important elements of this evidence, and to those having a special bearing on the present work.
Dental Caries
Historical Evidence
Dental caries was for nearly a million years virtually absent from ancient man [1] as it still is today from a few surviving primitive races and from wild animals. Furthermore, any caries that did occur was of a different type from that occurring in civilized man today, since it usually followed natural attrition of the teeth, or an injury to the dentine or cement, instead of arising as a direct attack on the enamel. [2, 7]
In this latter connexion, it is important to emphasize that the quality of the caries in a skull is almost as revealing as its quantity. Owing to the coarse foods consumed in bygone ages, the natural wearing-down of the teeth took place much faster than it does today, and most of any caries that did occur arose from food driven down into the narrow spaces sometimes appearing between the teeth during this process. Also, as the teeth wore down, the gum margins became more exposed to injury from fragments of bone etc. driven into them during mastication, and, again, caries could arise from food trapped in these areas. In each case the caries tended to occur near the necks of the teeth. The particles of food were too coarse to be trapped elsewhere. Today, however, owing to the refining of foods, caries mainly arises from minute particles trapped in tiny fissures in the enamel, or between the teeth just above their contact points. There is thus a big difference between the type of caries that occurred in former periods and that mainly occurring at the present time.
Though we cannot discuss in detail the very low incidence of caries in the Ancient Britons [3] (but flanked by a distinctly higher incidence in the more advanced civilizations of Egypt [4] and Greece [5] at that time), or do more than mention the rise in the incidence in Britain during the Roman occupation [6] and the fall that followed it, we must pause to give an illuminating contrast between the teeth in the Anglo-Saxons, after the departure of the Romans, and our own teeth today. Professor J. L. Hardwick [7] compared 1014 teeth in Anglo-Saxon skulls with the same number of paired teeth in patients in 1957. The result showed an incidence of caries Of 9.5 per cent in the former and 48.6 per cent in the latter. The distribution of the caries was also different, as already explained. The rise in caries since Anglo-Saxon times was relatively slow until the nineteenth century, [8] and then increasingly rapid, the significance of which will be seen in the next paragraphs.
There are few writers on the history of dental caries who do not consider that, although the disease has borne some relationship to the introduction of the practice of cooking food, its main march has been with the progressive removal of fibre in the refining of carbohydrates, [9] during the march of civilization itself. The removal of the fibre allows accumulations of carbohydrates to occur in and between the teeth, as we have just seen, in which fermentation by bacteria produces acids that attack the tooth structure. This attack by fermentative acids constitutes the essential caries process.
In the case of cereals it is a mistake to suppose that these refining processes are of a very recent origin. The practice of sieving out the bran from flour dates from quite early times. For example, apart from much earlier evidence from Egypt, [10] white flour was being produced in Greece at least as early as 500 B.C., and Hippocrates himself recommended white bread for a patient with diarrhoea, as we stated earlier in this work, thereby showing not only that white flour was being made then, but that it was already realized as passing through the gut at a reduced speed. [11] A quotation from Antiphanes, written before 350 B.C., shows that bakers were by that time producing white loaves in quantity, and by A.D. 50 the production of white flour was geographically widespread, [12] though socially confined to the higher grades of society in all the countries that produced it. In Britain, from the time of the Roman occupation, the flour was ever more frequently sieved to remove the bran. By the end of the sixteenth century white bread had not yet appeared in the cottages of the poor, but by the end of the seventeenth century some of the poor were eating it, and by the end of the eighteenth century practically all of them were doing so. [13] In the case of sugar, the refining processes, whereby sugar was first extracted from the sugar-cane and subsequently also from the sugar-beet, are of much more recent origin. Though sugar was produced in small quantities in the countries of antiquity, it did not reach England till the twelfth century, [14] and then remained a food of the rich for a very long time. The remarkable increase in its consumption, however, since the end of the eighteenth century is shown in Fig. 1 in Chapter II.
It would thus seem that the slow rise in the incidence of caries from the Bronze Age onwards was chiefly due to the refining of flour, but the much faster rise in recent times has been due to the refining of sugar. Though the starch in flour is converted by bacterial fermentation into sugar fast enough, any sugar eaten as such is clearly still more quickly fermentable into the final acids. Refined flour, however, through the removal of the bran, becomes much more sticky, owing to the concentration of the protein, and the resulting adherence to the teeth not only increases any fermentation from the flour itself, but also binds to the teeth any sugar eaten at the same time, and so increases the fermentation from that, too. Observing the soluble nature of sugar, such fermentation could not otherwise take place to the same extent. In connexion with the foregoing one might add that, owing to different ratios in the proteins present, refined rice when moistened does not become sticky like refined flour (which is the main reason why bread is not made from it), and therefore those races living on milled rice and very little else are singularly free from caries.
As an example of the shocking prevalence of caries in Westernized countries today, it may be stated that in Great Britain during 1963 there were provided to young people of 20 years of age and under no less than 5440 sets of full upper and lower dentures (including 640 replacements), and 84,330 courses of treatment which included the provision of partial dentures. To this total of some 90,000 dentures must be added dentures, mostly partial, supplied to 11,320 pupils by the School Dental Service, and still further dentures supplied under the Hospital and Specialist Services and a few under private contract. [15]
Racial Evidence
As an example of this evidence, the author in his first paper [16] drew attention to the remarkable deterioration of the teeth that has taken place in the inhabitants of the remote island, Tristan da Cunha, since 1932, [17] consequent on the arrival of refined carbohydrates in the island, which deterioration has been increasingly documented ever since. The Royal Navy has always had exceptional opportunities for medically observing the inhabitants of Tristan da Cunha.
The racial evidence in dental disease may also be exemplified by two quotations nearly 20 years apart.
In 1946: Professor J. C. Middleton Shaw: [18] ‘The native [of South Africa] in his natural state is not prone to dental disease, and there is little doubt that the primary cause of these diseases is the highly refined foods and sugars… .’
In 1964: Professor A. B. MacGregor, [19] after a recent survey of dental disease in Ghana, which showed the very close association between dental caries and refined carbohydrates, stated in his concluding remarks: ‘The significance of the survey lies in the fact that, while it has been postulated for many years that dental caries is associated with the consumption of refined carbohydrates, there is little direct evidence, and the evidence here presented was obtained from people living on the traditionally normal diet, some being able to afford refined carbohydrates and others not, so that reasonably controlled conditions could be obtained.’
Periodontal Disease
The loss of teeth from periodontal disease (so-called ‘pyorrhoea’) may, in some sectors of the community, rival the loss from caries itself, and often it seems that where the build of the teeth makes them more resistant to caries, the build of the gums makes them more prone to periodontal disease. This latter condition, also, is widely recognized as linked to the consumption of refined carbohydrates. As Sir Wilfred Fish [20] puts it in his work on this disease, the soft pappy nature of these foods does not provide sufficient friction to keep the gum margins hard and keratinized; any more than clerical work gives a person the hands of a bricklayer.
Considerable care, however, is needed in expressing the above view on the causation of periodontal disease. It is perfectly true that refined carbohydrates are a prime cause, but it does not necessarily follow that unrefined carbohydrates can not be a cause. It all depends on the form these unrefined carbohydrates take. If they take the form of stale, coarse, wholemeal bread, and hard fruits and vegetables, such as the raw apple, the fresh salad, and the fibrous vegetable, no periodontal disease will follow their consumption. But if they take the form of boiled whole grains, such as soft porridges of maize or oats, and various vegetable mashes, with little other food eaten, then periodontal disease may still supervene. This happens in many natives in India and Africa, where the diet is of just this type, whereas Eskimoes and Australian Aborigines, who eat little carbohydrate but much tough meat, escape. It is clear from the above that, where periodontal disease is concerned, unrefined carbohydrates have every advantage over refined carbohydrates, but some of them should be eaten in the raw state. To summarize, those who eat unrefined carbohydrates are candidates for salvation over periodontal disease; those who eat refined carbohydrates never are.
At this point a few lines must be devoted to the subject of dental plaque. If, in the presence of a refined diet, the teeth are not cleaned with a toothbrush for several days, many people can actually sense a film forming over the teeth. This film, or dental plaque, a large part of which in Nature is kept removed by the friction of hard fruits and vegetables, has sinister dental implications. Not only does it harbour to a dominant extent the bacteria responsible for caries, but it also plays a big part in the initiation of periodontal disease, just described.
As regards caries, some micro-organisms in dental plaque are capable of producing from sucrose various extracellular polymers, largely dextrans, which, being sticky, favour the extension of the plaque. These extracellular deposits also act as a reservoir of fermentable material for the organisms, with consequent maintenance of the carious process over longer periods of time. And as regards periodontal disease, such a chain of events in dental plaque, when occurring near the gum margins, produces a direct inflammatory effect on the gums themselves, which is aggravated by any mechanical injury arising from roughened enamel surfaces, or the sharp edges of cavities, due to the carious process. This gingivitis is the essential initiator of periodontal disease.
The author here wishes to record his gratitude to Professor J. L. Hardwick for his great assistance over the subject of dental plaque and the origin of periodontal disease.
Fluoridation of Drinking Water
It is not intended to discuss this issue, except to point out that the prevention of dental caries is no more important than the prevention of the dreaded periodontal disease, or, for that matter, of most of the other saccharine manifestations set out in this work. And however useful fluoridation is in the prevention of caries, it can do nothing for the prevention of periodontal disease or of these other manifestations. Therefore, the prevention of caries, by removal of the cause, alone appears to hold out any hope of success in this wider sense. And that means educating the public to the dangers in eating refined carbohydrates, so that their consumption is drastically reduced, especially in school tuckshops, as referred to in the final chapter.
What can, indeed, be achieved by removal of the cause in the case of the dental diseases discussed here is well seen in the two-year study, 1955-7, by G. L. Slack and W. J. Martin, [21] in which schoolchildren were given slices of apple after meals. These children, as long as they were given the slices of apple, not only got significantly less caries than the control children did, but they got much less gum disease, too. To the purely dental result could be added the reduction in potential other disease that follows from the evidence presented in this work. It is into educative channels of this type, plus some subsidization of school tuckshops to sell fruit, nuts, raisins, etc., instead of sweets, that fluoridation costs would seem better directed.
References
1. National Research Council, Washington, D.C. (1952), Survey of the Literature of Dental Caries, 127. Publication 225.
2. Colyer, J. F., and Sprawson, E. (1953), Dental Surgery and Pathology, 9th ed., 383-384. London: Butterworth.
3. Ibid., 317-318.
4. Ibid.
5. Kirkos, A. (1935), Trans. Amer. Dent. Soc. Eur., 174, 7.
6. Hardwick J. L. (1960), Brit. Dent. J., 108, No. 1, 9.
7. Ibid., 11, 12.
8. Ibid., 13, 14.
9. Colyer, J. F., and Sprawson, E., Op. cit., 386-391.
10. McCance, R. A., and Widdowson, E. M. (1956), Breads, White and Brown, 2. London: Pitman Medical.
11. Ibid., 9.
12. Ibid., 6.
13. Ibid., 46.
14. Hardwick, J. L., Op. cit., 12.
15. From figures kindly procured for the authors by G. W. Marshall, British Dental Association, from the Ministry of Health.
16. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 42, No. 2, 55.
17. Gamblen, F. B. (1953), Ibid., 39, No. 4, 252.
18. Shaw, J. C. Middleton (1964), S. Afr. Dent. J., 20, No. 8, 238.
19. MacGregor, A. B. (1946), Ann. R. Coll. Surg. Engl., 34, 179.
20. Fish, E. W. (1946), Paradontal Disease, 18. London: Eyre & Spottiswoode.
21. Slack, G. L., and Martin, W. J. (1958), Brit. Dent. J., 105, No. 10, 366.
Chapter VI
Obesity
I. General Considerations
THE type of obesity to be discussed here is the ordinary idiopathic or ‘essential’ type, and not those exceptional types associated with damage to, or tumours of, the diencephalon, or with disease of one of the ‘target’ endocrine glands. The author considers that such obesity is one of the most obvious manifestations of the saccharine disease, the single primary cause lying in the consumption of refined carbohydrates. As already shown, the refining processes lead to unnatural concentration in the carbohydrates concerned, which deceives the tongue and the appetite, and leads to over-consumption — and this over-consumption is the sole primary cause of the overweight. With unrefined, unconcentrated carbohydrates over-consumption does not occur, and obesity does not occur either, as the author intends to demonstrate.
This line of reasoning positively excludes as a primary cause of obesity any fault in the instinct of appetite (such as the mysterious derangement, postulated by some, of a hypothetical ‘appestat’ centre in the brain); it likewise positively excludes as a primary cause any dislike of, and consequent abstention from, taking exercise. In short, it is advanced that, as regards obesity, the body, again, is not built wrongly, but is being used wrongly.
To refer to the two causes just rejected, the view that in obesity the appetite is at fault can easily be assailed. There is first of all the general evidence. In holding the view that the body is often imperfectly evolved over this instinct, the holders are faced with the incidence figures. Once again it may be stated that no known hereditary defect occurs more often than five times in one thousand births. How often does obesity occur? Besides, if the condition were a hereditary defect, the age of onset would tend to be different.
Then there is the specific evidence. A glance at any wild creature in its natural environment shows that no matter how plentiful its food supply, it never cats too much of it. Even a poulterer’s shop reveals that no wild rabbit ever ate too much grass, no wood-pigeon ever ate too much wheat, and no herring ever ate too much plankton. No wild creature, in fact, is ever overweight. The forces of evolution have ensured that in nature organisms react to an abundant food supply never by developing a disease, such as obesity, but by raising the rate at which they propagate themselves. This is true for the whole of creation, from a lactic acid bacillus in a bottle of milk right up to man himself in circumstances of plenty. In Part II of this chapter it will be shown that the freedom from obesity in organisms living under natural conditions applies equally to man, as will be seen shortly in Africans living tribally on unrefined foods.
The view that obesity is due to insufficient exercise is just as vulnerable. In the first place, the lack of exercise held responsible is nearly always a voluntary lack, not an imposed lack. People are blamed for using lifts in office buildings and for not walking when they leave their offices. Yet this is what their natural inclinations often tell them to do. Some don’t want to climb stairs, and don’t want to go walking either; they would rather sit down when they get home and put their feet up. Therefore the argument that this instinct is wrong is just as vulnerable as the argument that the instinct of appetite is wrong. Throughout the whole animal kingdom, in fact, no living creature, unless forced to do so in order to get food, ever takes any more exercise than it wants to take. Nature obviously likes to conserve the heart — and certainly never inflicts on any organism the penalty of obesity for ‘laziness’.
Even in cases of imposed lack of exercise obesity does not occur as long as the food is not tampered with. A visit to any zoo will show this very clearly. Here will be seen the two opposite poles of creation — a large animal like a tiger, accustomed to hunt its prey over many square miles of jungle, and now confined to a space measured in cubic feet; and a small bird, like a finch, accustomed to fly about many acres of countryside, and now confined to a space measured in cubic inches. In each case the natural exercise has been enormously reduced. Yet, just because each of these creatures continues to take its food in its natural form, in the one case raw meat and bones, and in the other case unaltered seeds, the weight remains the same and obesity does not occur.
An exception to this appears to exist in the fattening up of animals and birds for market. But a closer examination will nearly always reveal in these circumstances either that food concentrates have been given, in which case the whole argument instantly alters, or that the animal or bird is of a kind that has been evolved by selective breeding over many centuries to become much fatter than its wild counterpart. For example, in the Pekin (Aylesbury) duck the bird’s muscles have been so replaced by fat that it is never able to fly off the ground. Finally, what is under discussion in humanity is not an imposed lack of exercise of this sort, but a voluntary one. No one in this country is prevented from taking exercise if he wants to. The point is that he often doesn’t want to, and the present argument then applies.
It is therefore contended that the sole cause of obesity lies in the consumption of refined carbohydrates. A large appetite is not a cause, and a dislike of exercise is not a cause. These points have all been stressed in the author’s past writings, as also have those below.
It is perfectly true that restraint of appetite or enforcement of exercise will reduce obesity, but as long as the true cause continues to operate — the consumption of refined carbohydrates — the use of either is an example of two wrongs not making a right. To be sure, these two factors are valuable in the removal of surplus weight already in existence, but in the basic matter of prevention the mind should be riveted on the essential cause and not confused by irrelevancies.
Equally, it should be thoroughly realized that unrefined carbohydrates, such as wholemeal bread, potatoes eaten in their skins, [1] raw fruit, etc., are no more fattening than any other natural food, including protein foods and fatty foods. Some starvation for established excess of weight is clearly indicated, but a distortion of the personal choice of the various classes of foodstuffs, except for the omission of fats, is emphatically not.
Finally, it will be realized that in this conception obesity is not due to diabetes, nor diabetes to obesity, but both arise from a common cause. Whether the one condition occurs, or the other, or both together, depends on the personal make-up in the individual concerned, in the presence of the unnatural environmental factor, held here to be the consumption of refined carbohydrates. In this respect there is no fundamental difference between the association of obesity with diabetes and, say, its association with gall-stones, coronary thrombosis, or any other manifestation of the saccharine disease.
II. Racial Studies
The author is indebted to Dr. G. D. Campbell for pointing out the rarity of obesity in Zulus living tribally, on a diet substantially unrefined, as opposed to its commonness in urban Zulus living on a diet of much more refined type. These differences in the two groups of Zulus have been fully documented by C. Slorne and others, [2] who at the time of making their study were members of the Department of Sociology and Anthropology of the State College of Washington, U.S.A., and to whose meticulous paper those interested are referred. The absence of obesity in humanity wherever still living on natural, unrefined foods has indeed been so often observed that it is not necessary to pursue the matter here, and we therefore pass on to a more important consideration.
III. Treatment
From the argument presented above, it is clear that the treatment of obesity lies in the same fundamental step indicated in the other manifestations of the saccharine disease — the avoidance of refined carbohydrates. This treatment may be summarized in the case of obesity as ‘seeking safety in dilution’ — the dilution present in natural carbohydrates, through the existence of fibre. There are three points to be noted:
- In the matter of the prevention of obesity, and in the early stages of the condition, the above is all that is required, but for established cases a certain amount of starvation will at first also be necessary, such as the omission of breakfast and afternoon tea. However, as already explained, the natural pattern of the diet should not be distorted by substituting fats for carbohydrates. On the contrary, since, as the author hopes to have shown, unrefined carbohydrates are not fattening, any distortion of the natural pattern should lie in specially reducing the fats, since this forces the body to consume its own excess of these. The proteins, needless to say, are never a target of interference.
- Naturally desired exercise is encouraged, but forced exertions are not. The reasons for this have already been set out.
- The author has found that a careful explanation to the patient, of how Nature has been deceived, in the production of obesity, is of the greatest assistance. An intelligent person, looking around at the rest of creation, will recognize the truth for himself, and will then largely be in command of his own fate. It is, indeed, most advantageous that patients should have confidence in their own judgement in this way, rather than be obliged to accept edicts laid down by others. These points are largely covered in the diet card at the end of this book.
It will be noted that the fundamental difference in the present approach to obesity, from that based on the supposed faulty functioning of an ‘appestat’ centre in the brain, is that the appetite is not regarded as an enemy here, to be placed in a strait-jacket, but as a normal instinct, to be let loose on foods so naturally diluted by fibre that the instinct is neutralized in a natural manner. Hence the emphasis on crude wholemeal bread several days old, raw fruit such as the apple, and bulky vegetables, in the diet card just referred to. To the author, holding the line of reasoning that he does, it is anathema to try to antidote a supposed derangement of an appestat centre in the brain by filling the stomach before a meal with a substance like methyl cellulose. In his reasoning the only production of distension in the stomach to be considered is the distension produced by natural fibre in natural foods.
It will also be noted that the present approach is quite distinct from that of J. Yudkin, referred to in Chapter II, which regards many natural carbohydrates as an enemy, and leads to assessment of the danger in individual carbohydrates by their calorific value. [3] It is perfectly true, as has been shown previously (Chapter II), that the calories in, for example, an apple are much the same as those in a teaspoonful of sugar, and therefore at first sight the danger in cases of obesity would appear to be the same in each. But, as was pointed out, there is an enormous difference between the two in one vital respect — the amount a person needs to consume of each before the appetite is appeased. As already said, a person may over-consume sugar very easily — but not apples. In this distinction is seen nothing less than the difference between satisfaction and craving; between following a régime and departing from it; between obesity and no obesity. In the author’s opinion the danger in carbohydrate foods should be assessed not by their calorific value, but simply by whether they are natural or refined.
At the same time considerable care must be exercised in deciding whether a carbohydrate food is natural, even if it is unrefined. For example, at first sight, honey, and certain fruits such as dates, would appear to be natural foods. A deeper look at these foods, however, considerably modifies this view. Until very recent evolutionary times honey, in fact, has seldom been available at all. It is true that ever since the discovery of fire mankind has in theory been capable of smoking out the nests of wild bees, and there is the archaeological evidence that he occasionally did this. A little reflection, however, will show that such a feat must have been an extremely difficult one to bring off, and in any case would have yielded so little reward as seldom to have been worth the effort. To the consumption of honey, which contains practically no other food material than sugar, man is therefore little more adapted than he is to that of sugar itself, as sold in grocers’ shops, and anyone arguing that honey is a natural food, which he can eat ad libitum, is in for some nasty surprises. Solomon may not always have been wise, but he certainly showed his wisdom in advising people to keep off much honey (Proverbs XXV. 27). In short, honey should be regarded for practical purposes as being as dangerous as sugar. This applies to all the manifestations of the saccharine disease and not only to obesity.
As regards dates, these certainly are a natural food — but not for the white races! In the date the sugar present is enormously concentrated. Thus, if the percentage of sugar present in the apple is about 10 per cent, and in the banana 20 per cent, in the date it is 60 per cent. In the white races such concentrations can easily deceive the tongue and the appetite. The same applies to certain dried fruits if consumed by themselves, such as raisins, which have a comparable sugar content to that of dates; and in fact the banana, with a sugar content of 20 per cent, which exceeds that of all the natural fruits of the British Isles, represents the rough limit of safety in this respect. Needless to say, the circumstances become much altered when these concentrated fruits are diluted by other natural foods, as currants are in a wholemeal currant loaf. Then, except where the obesity is very marked, they become desirable, since they lead to the avoidance of the much more dangerous sugar itself. Similarly, dates, or for that matter bananas, are best consumed with a glass of milk (with which either forms a most palatable combination), the tongue alone deciding for any given person the ratio of either fruit to the milk taken.
Arguing on the same lines as the above, it is clear that potatoes can only be allowed if boiled with their skins on, and the skins eaten. It is also important that people be warned that beer and other malted liquors, though they do not taste sweet, are — through their content of malt sugar — as fattening as any foods that exist. If alcohol must be taken by the obese, it should be taken in other forms than beer, which definitely counts as a refined carbohydrate.
In conclusion, the author may say that he has never been let down over the above natural approach to the treatment of obesity, and he hopes that the diet card at the end of the book may prove to be of help to those prepared to think deeply. If he were asked why the treatment of obesity is so often fraught with difficulty, he would say: ‘Because people’s minds are being directed towards calories instead of to the basic cause — the unnatural concentration present in sugar and white flour. And also because the prevention and arrest of obesity is infinitely easier than the removal of obesity already in existence (but in which the basic approach still holds).’
References
1. Cleave, T. L. (1962), Peptic Ulcer. Bristol: Wright.
2. Slome, C., Gampiel, B., Abrahamson, J. H., and Scotch, N. (1960), S. Afr. Med. J., 34, 505.
3. Yudkin, J. (1960), This Slimming Business. London: MacGibbon & Kee.
Chapter VII
On the Causation of Diabetes
I. Preliminary Considerations
SOME twenty years ago, that is, in 1955, if the incidence of diabetes was being related to the consumption of any particular class of foodstuff, it was being related to the consumption of fats. This was largely due to a paper by H. Himsworth (1949), [1] who showed that during the 1939-45 war, when the diabetes mortality fell steeply in all the countries that experienced food-rationing, the only class of foodstuff to show a coincident fall in consumption was the fats; the carbohydrates and proteins showed an actual rise. After demonstrating this relationship, Himsworth continued: ‘There is a mass of evidence with similar import. The progressive rise in diabetic mortality in Western countries during the last fifty years coincides with a gradual change towards higher fat and lower carbohydrate diets; the protein and caloric values have altered little… But that is not to say that fat is the deleterious factor; it may simply serve as an indicator of other and more important contingent variables.’
Fig. 5 shows the relevant chart for the 1939-45 war from this paper.
 Fig. 5. — England and Wales food consumption and female diabetic deaths. Showing the correlation between food consumption and diabetic mortality rate. The female rate was chosen as less influenced by mobilization, and the curve antedated one year to allow for time lag. (Himsworth.) |
In a paper around that time (1956) the present author [2] contested the above relationship of diabetes to fat consumption, on evolutionary grounds. Using the argument set out in Chapter II of the present work, he pointed out that carbohydrates should not be taken as a single group but as two very different groups; one being natural, unconcentrated carbohydrates, such as unrefined grains, potatoes, and fruits, and the other being unnatural, concentrated carbohydrates, notably refined flour and sugar. And that as the body was evolved to the consumption of natural carbohydrates, no harmful over-consumption of these would occur, no matter how much of them might be needed to satisfy the calorific requirements; whereas the opposite was true of the refined carbohydrates, which were only too likely to be over-consumed — especially in the case of sugar, which is many times more refined than even the whitest flour. And that such over-consumption, especially of sugar, imposed a pathogenic strain on the pancreas and was the essential cause of diabetes. This argument enabled the most logical of all foodstuffs to be causally related to the disease.
Turning specifically to the 1939-45 war, he pointed out that if there were charted against the fall in diabetes mortality, not the consumption of all carbohydrates, but only that of the refined ones, then, with the great replacement of sugar and white flour by coarse flour and potatoes as the war proceeded, the chart would show a considerably greater fall in the case of the former (sugar and white flour) than in the case of fats, and what was the opposite of a relationship between the diabetes mortality and carbohydrate consumption would become a very close relationship. Reproduced here, in Fig. 6, is such a chart, involving the consumption of sugar, which is by far the most important member of its group. (It should be added, however, that with the discovery of penicillin near the end of the period, and with the introduction of the newer insulins, the diabetes mortality did not follow the rise in sugar consumption that took place with derationing in subsequent years. This would apply equally to Himsworth’s postulated relationship between the mortality and fat consumption, when the latter also rose with derationing.)
 Fig. 6. — England and Wales. Diabetic mortality indices (1938 basis). The figures for 1946 and 1947 have been kindly supplied by Dr. Percy Stocks. After Himsworth, with curve of sugar consumption (broken line) superimposed. (Drawn by T. L. Cleave.) |
In his paper the author then applied the above argument to the rest of Himsworth’s contention, pointing out how any increase in the consumption of fat in Western nations must, for evolutionary reasons, have been small indeed by comparison with the increase in the consumption of sugar, this latter being of a magnitude to match the increase in the mortality of diabetes itself — which, starting around the middle of the nineteenth century, progressed to such an extent that the disease, from being twenty-seventh in the list of causes of death in the statistics of the Metropolitan Life Insurance Company in 1900, became the third commonest cause by 1950. He also pointed out the relative rarity of diabetes in rural China and India, where most of the inhabitants do not yet show the food-sophistication exhibited by the West.
The author elaborated the whole of the above argument in a later work, on Peptic Ulcer (1962), [3] from which quotations will now be made, showing how certain objections that could be made to this line of reasoning may be overcome.
‘As regards the decline in the incidence of diabetes during the war, the food shortage at that time caused a big fall in the consumption of fats and a corresponding rise in the consumption of carbohydrates. It is true that these latter were eaten relatively unrefined, mainly in the form of grain and potatoes and including little sugar, but since all the starch in carbohydrates is itself digested to, and absorbed as, sugar (glucose), it is clear that during the war the ultimate absorption of sugar in the belligerent peoples was higher than ever. How, therefore, can diabetes be related to the consumption of refined carbohydrates, especially sugar? Qualitative differences in sugar absorption were referred to in Chapter II and do not affect the present argument.
‘Again, as regards the virtual absence of diabetes in primitive communities, these communities are usually ones that live almost entirely on carbohydrates, such as various grains and tubers. It is true that the carbohydrates are eaten substantially unrefined, as in the form of whole maize or millet, or home-pounded rice, but again, since all the starch contained in these is digested to, and absorbed as, sugar, it is clear that the ultimate sugar absorption in such communities, which do not eat refined carbohydrates, is higher than in civilized peoples, who do.
* * *
‘The best way to expose the fallacy in these arguments is to consider another condition altogether — dental caries. It is accepted everywhere that this condition is related to the consumption of refined carbohydrates, especially sugar. During the last world war, for example, a big fall in the incidence of caries occurred in all the belligerent countries, pari passu with the fall in the consumption of these refined products; also, in communities all over the world caries is slight or absent until these products appear amongst them, a recent striking example of this being provided in the inhabitants of Tristan da Cunha.
‘This overwhelming epidemiological evidence quite rightly ignores the fact that during the war the total carbohydrate consumption in the belligerent countries went up, and that amongst communities which get little or no caries the total carbohydrate consumption is nearly always much higher than amongst civilized peoples who get a great deal of it. For what matters in the production of caries is not the quantity of carbohydrates consumed, but the form in which they are consumed — to be more accurate, whether they have been refined or not. A whole cartload of carbohydrates in the form of raw apples or sugar-beet, for example, would do the teeth nothing but good, whereas a few cases of refined, sweet biscuits, leaving a sticky residue around the teeth, could initiate the fermentative process responsible for decay and therefore do the teeth great harm.
* * *
‘Exactly the same argument, though involving a different pathogenic mechanism, is applicable to the causation of diabetes. Here also what is concerned is not the quantity of carbohydrates consumed, but the form in which they are consumed, i.e., whether they have been refined or not. There are two ways in which the consumption of refined carbohydrates could strain the pancreas, and all other instruments of sugar metabolism present in the body, and lead to the development of diabetes.
- ‘Direct over-consumption of these carbohydrates, through deception of the tongue and appetite, as already explained, the over-consumption being measured not simply by the total amount of carbohydrates consumed, but by the total amount consumed relative to the total amount needed (for conversion into heat and mechanical energy at that time).
- ‘Another way is to assume that what strains the pancreas is what strains any other piece of apparatus — not so much the total amount of work it is called upon to do, but the rate at which it is called upon to do it. In the case of eating potatoes, for example, the conversion of the starch into sugar, and the absorption of this sugar into the blood-stream, is a much slower and gentler process than the violent one that follows the eating of a piece of Brighton Rock, for example, or other mass of concentrated sugar.’
In this connexion D. G. Campbell (1971, in Diabetes, Proc. 7th Congress Internat. Diab. Fedn., page 328. Amsterdam: Excerpta Medica) has recently produced a series of blood-sugar curves, showing how violent is the rise after eating neat sugar, compared with the gentle undulations after eating the same calorific value of carbohydrate in the form of the natural apple and potato. Even peeling the potato, which brings it into the refined category, and which the present author has long maintained is the only reason why potatoes have acquired a bad reputation in obesity, as set out in the previous chapter, makes a noticeable difference in the blood-sugar curve.
It is thus easy to understand that in the belligerent peoples during the war, as in primitive communities today, the stresses imposed on the pancreas, in spite of a large consumption of unrefined carbohydrates, were much less than in Westernized peoples at the present time. These, taking some 5 oz. of refined sugar per head per day, can often consume in a matter of minutes material that, in its natural form (for example, some 2-1/2 lb. of sugar-beet or up to a score of ordinary apples), would normally be eaten over several hours.
* * *
It is seen, therefore that the two objections to the present conception, noted above, can be met, and if the present writer’s labours have achieved anything of value in diabetes, it is the elucidation of the absolutely crucial distinction, in all epidemiological studies of the disease, between the consumption of refined and unrefined carbohydrates.
From these preliminary considerations it will be clear that the author holds that the cause of diabetes lies essentially in the consumption of refined carbohydrates, which imposes unnatural strains upon the pancreas, either through over-consumption, or through rapidity of consumption and absorption, or through both.
At this point the author must stress that this work is concerned with the evolutionary and epidemiological aspects of the conditions studied, not the pathological ones. He therefore has no intention of entering the ever-changing labyrinth constituted by the pathological aspects of the pancreatic strain just mentioned. It would seem, for example, that anti-insulin may be no more than a natural response of the body to free insulin in the blood, appearing after injections of this substance in the treatment of diabetes.
The author will endeavour to show later that the hereditary features of the disease, which are undoubted, do no more than reflect the inheritance of personal build, including that of the pancreas itself, rendering the persons concerned more vulnerable to the new environmental factor; and that these features in no sense indicate hereditary defect. In short, to use the previous commonplace expression, he will try to show that the body is not built wrongly, but is being used wrongly.
II. The Incubation Period in Diabetes
The incubation periods in the various manifestations of the saccharine disease have already been discussed (Chapter II), and before dealing with certain epidemiological features in diabetes it will be desirable to refer to the incubation period of this particular manifestation. In 1959 G. D. Campbell [4] showed that there seemed to be a remarkably uniform period in a population exposed to a diabetogenic factor in their midst, before the disease itself appears amongst them. This period was formulated as ‘The Rule of Twenty Years’. The rule was first worked out in the case of the urban Zulu, with incrimination of sugar as the factor most likely to be involved, the data being published later in the South African Medical Journal, in 1960. [5]
The rule of 20 years has since been supported by other writers in other countries, as will be seen in the case of V. Albertsson in Iceland and A. M. Cohen in Israel.
If the present author were asked how he would reconcile a 20-year incubation period in diabetes with the rapid drop in mortality he has just shown as occurring during the sugar rationing of the last war, his reply would be as follows (and this indeed was given in the earlier joint work): What is involved here is a reduction in the final spill-over of accumulated pathology into the production of overt disease, when such accumulation can no longer be held latent by the body’s efforts in compensation. If the cause is removed, this spill-over can be stopped at once, though the accumulated pathology remains and may spill over later, as the body’s compensatory mechanism ages (just as occurs in some other diseases, such as cancer of the lung due to smoking). And if all this is true of supposed new cases of diabetes, it is also true of the mortality which actually occurred. For, as regards stages of development, death is to overt disease as overt disease is to latent disease.
It is important to add that an incubation period of 20 years in the case of diabetes makes it impossible to argue, as E. P. Joslin [6] does, against the consumption of sugar being a cause of diabetes because ‘in the United States the consumption of sugar has been stationary in recent years, whereas diabetes has increased; and in certain other countries, where the consumption of sugar is high, the incidence of diabetes is relatively low’. Countries with a present high sugar consumption, of fairly recent origin, as in the case of developing countries, may face an outbreak of diabetes in 20 years’ time. This, indeed, is exactly what is happening in the Canadian Eskimoes today. Joslin also supports his argument with figures of the mortality from diabetes. Now the rule of 20 years concerns incidence. If the rule concerned mortality, it might well have to be altered to a rule of 40 years, since it would depend on how long diabetics lived after their condition was diagnosed. And that, again, would depend on the efficacy of the treatment in the country concerned. Viewed against the background of the present rule, therefore, let alone its extension, the second part of Joslin’s argument is seen to be just as assailable as the first part.
III. Racial Studies: Africa and India
In the previous joint work, already alluded to, the above view on the causation of diabetes was strongly supported by racial studies, including those carried out in Natal by Dr. G. D. Campbell, [7] aided by Dr. E. L. Batchelor, which showed, on the one hand, a very high incidence of the disease in a large number of the descendants of past immigrants from India (the ‘Natal Indians’ numbering some 400,000 persons) and, on the other hand, a very low incidence of the disease in native Africans, of the Zulu tribe, still living in the tribal manner on unrefined carbohydrates (largely maize). These incidences of diabetes were matched with studies in sugar consumption, which in the Natal Indians is very high, but which in the tribal Zulus has always been very low, though in recent years there has been a spectacular rise (for example, from 6 lb. per head per year in 1953 to 60 lb. in 1964). It is to be noted, however, that past incidences and past consumptions, when compared with present ones, are often the most revealing studies of all, and the full. value of these studies may have yet to be seen; as stated earlier, they invite pursuit, either in the joint work or in the original papers.
(It may be added parenthetically, for later reference, that Dr. Campbell’s studies also showed that the fat consumption in the Natal Indians mainly consisted, not of animal fats, but of vegetable oils, largely unsaturated, and yet the incidence of coronary disease in these people is almost as striking as the incidence of diabetes.)
Meanwhile, the incidence of diabetes in India itself is far lower, as set out in the joint work, in keeping with a far lower sugar consumption, too (some 12 lb. per head per year, [8] against at least 60 lb. in the Natal Indians [9] ). It is also important that the incidence of diabetes in India is much higher in the southern parts, where the staple food is milled, white rice, than it is in the northern parts, where the staple food is unrefined wheat and maize. Indeed, as regards the latter areas, personal communications to the present author in 1964 from Dr. J. G. H. Shaw and Dr. T. C. Skinner, from Mission Hospitals at Peshawar and Jalalpur Jattan respectively, state that diabetes is rarely seen there amongst the country-dwellers living on these unrefined foods, the admission rate for diabetes at the latter hospital, for example, during 1957-71 averaging only 1 case per 1000 admissions. Meanwhile, in the town-dwellers in Chandigarh and Amritsar the incidence of diabetes is much higher — but then the sugar consumption is higher, too, a suggested figure [10] for Chandigarh being up to 4 lb. a month, which is much above the national average. It may be added here that however possible it is to relate diabetes in India to the consumption of refined carbohydrates, notably milled, white rice, it is normally impossible to relate it to the consumption of fats, for the Indian Council of Medical Research [8] has shown that in the masses of India the fat consumption is only half that considered necessary for the preservation of health.
Before leaving the subject of diabetes in India, it is significant, with reference to the clinical association of the various manifestations of the saccharine disease with each other, that the regions of highest incidence of diabetes are also those of the highest incidence of peptic ulcer — the so-called ulcer belt in the southern part of India, where, as just said, the staple diet is milled, white rice. This subject will be pursued in Chapter X, on peptic ulcer.
It is also important to add that obesity, so rare amongst the masses in India, is very common amongst the masses in the Natal Indians.
Finally, to refer back to the rarity of diabetes in Africans living tribally, which is everywhere admitted, the incidence of the disease in urban Africans is, by contrast, reaching equality with that in the whites, [11, 12] just as it already has done in the cousins of these Africans, the Negroes in the United States, [6] where the diet closely resembles that of the whites.
A further point, which is of the utmost importance, is that the Zulu and Pondo cane-cutters in Natal, who have always been allowed to chew as much sugar-cane as they please, have been shown to be singularly free from diabetes — indeed in over 2000 of these cane-cutters tested by Dr. Campbell [7] and his colleagues, all that has been found is a trace of sugar in the urine in 3 of them, which supports the contention that the consumption of unrefined carbohydrates is as harmless as that of refined carbohydrates is dangerous, assuming the former are eaten by the indigenous inhabitants.
This observation from Natal is in striking agreement with a statement of F. G. Banting, co-discoverer of insulin, in the Edinburgh Medical Journal, vol. 36, of January, 1929: ‘In 1924, while visiting Panama, I was told by Dr. Clarke, pathologist of the Ancon Hospital, that on examining 5000 men who were applying for work on construction of the Panama Canal he had only found reducing material in the urine in 2 cases. Neither of these cases proved to be diabetic. This is the more remarkable because a large percentage of the labourers were natives of Dominica, where a main article of diet was sugar-cane. From the time the children are weaned until they die they eat the sugar-cane. There are also wealthy Spaniards living in Panama who eat large quantities of refined cane sugar. Indeed much of their food is cooked in syrup. The incidence of diabetes amongst this class is surprisingly high.’ [13] Dr. G. D. Campbell brought this valuable reference to light.
It should be added that the above cane-cutters in Natal are now receiving a supplementary ration of refined sugar, and it will be interesting to see if their incidence of diabetes changes in the future.
IV. Other Racial Studies in Diabetes
It will now be convenient to relate diabetes to the consumption of refined carbohydrates in some other communities and countries, to supplement those already quoted. Actually, the present author knows of no country where this relationship cannot be established, always assuming the following:
- The consumption of unrefined carbohydrates, such as sugarcane, must be carefully weeded out. The importance of this has already been shown.
- The incubation period must also be carefully allowed for, as already set out.
- The consumption of refined carbohydrates must embrace all types of these, including not only refined sugar, but also refined (white) flour, polished rice, and in some countries even manioc or cassava (tapioca). Malted liquors such as beer, and many native brews, must certainly also be included in the consumption of refined carbohydrates. For malt sugar is a particularly significant example of these foods, and the errors that occur if its consumption is disregarded are discussed in detail in Chapter VIII, on coronary disease. All refined carbohydrates are liable to be consumed in excess, as explained in Chapter I, and, since all are absorbed as monosaccharide sugars, are liable to affect the blood-sugar curve to an unnatural extent, either in height, or in speed of ascent, or in both. But, being unnaturally concentrated to a greater extent than any other refined carbohydrates, table sugar, whether white or brown (demerara), is always the most serious in the production of disease.
a. Trinidad
The importance of considering the consumption of all refined carbohydrates is well seen in the incidence of diabetes in Trinidad. Thus, T. Poon-King [14] and others have pointed out that the incidence of the disease in that island was 2.37 per cent in the East Indian inhabitants, but only 1.44 per cent in the Negro inhabitants. Yet the sugar consumption in the two groups was almost identical at 47-48 g. per day, so the difference in incidence could not be related to sugar consumption. However, if refined cereals are also considered, the picture changes at once, for the consumption of these shows an average figure of 379 g. for the East Indians but a figure of 287 g. in the Negroes. The present author was in Trinidad during the Second World War, and knows it well and the multiracial society of which it is composed. After reading the above Lancet paper, he took the opportunity to revisit the island and meet Dr. Poon-King, who afforded him great help in exploring the figures given in his article and in establishing the point now being made.
b. The Eskimoes
In the previous work implicating the saccharine disease, the present author considered the incidence of diabetes in Eskimoes was lower than would be expected from their exposure in recent times to refined carbohydrates,, and it was suggested that if this lower incidence became confirmed, it might be explained by their lesser liking for these foods, owing to the normal lack of them in their natural environment. Time has since shown, however, that this explanation is unnecessary, because the lower incidence of diabetes has not been confirmed. Indeed, with the greater availability of sugar and white flour, the consumption of the former substance amongst Canadian Eskimoes has now risen to over 100 lb. per head per year [15] and, with the expiring of the 20-year incubation period already discussed, diabetes [15] is now commonly occurring amongst them. The same is true of other manifestations of the saccharine disease, in these people, such as gall-stones, etc., already set out in Chapter II.
However, as regards the more remote Greenland Eskimoes, the situation is much the same as existed amongst their Canadian cousins a decade and more ago, the consumption of sugar being still very low and the incidence of diabetes correspondingly low, too. [16] But the sequence that has occurred amongst the Canadian Eskimoes appears only too likely to follow amongst the Greenland Eskimoes, in which case the same sequence in the two groups will not only be evidence of diabetes being a manifestation of the saccharine disease, but perhaps also the strongest of any such evidence that exists.
The author is particularly indebted to personal communications from Dr. O. Schaeffer of the Charles Camsell Hospital, Edmonton, Canada, and from Dr. H. O. Bang of the Aalborg Hospital North, Denmark, for many personal communications on the Canadian and Greenland Eskimoes respectively, on whom they have performed such valuable studies.
c. Cherokee Indians
Professor K. M. West and others, [17,18] of the University of Oklahoma, U.S.A., have made a study of diabetes in certain racial groups. These groups included natives of the working class in East Pakistan (now Bangladesh) and the Cherokee Indians of North Carolina, U.S.A. Both these groups are of interest, because in each group the diet consists mainly of carbohydrates, and refined carbohydrates at that, but whereas the carbohydrates in the former group consist mainly of rice, with very little sugar, the carbohydrates in the latter group consist mainly of white flour, with large amounts of sugar.
In these studies, in each case on about 500 subjects over the age of 30 years without known diabetes, and matched as closely as possible, the incidence of the disease, as based on arbitrary blood-sugar criteria, was 1.5 per cent in the East Pakistanis and 26 per cent in the Cherokees. This difference is supported clinically by the vastly greater number of cases sent to hospital in the latter group. In the previous joint work it was shown that hospital admissions for diabetes in India average about 1 per cent. A personal communication from R. Bokat (1965), Director of the U.S. Public Health Service Hospital at Cherokee, forwarded by Professor West, to whom the author is greatly indebted for many personal communications, shows that the admissions for diabetes there average 12 per cent. Incidentally, for adult admissions only, the average is about double this — 25 per cent. The question of inbreeding as a factor in this very high incidence is under discussion.
To turn back now to the diets, though in the paper no breakdown is given of the carbohydrates consumed, which supply the bulk of the calories in each case, we may assume that, as the Cherokees are living in the United States, where sugar consumption exceeds 100 lb. per head per year, the difference in the consumption of this particular foodstuff by these two groups will be very great, as it has already been shown in Part III, above, that the average sugar consumption in India is only about 12 lb. per head per year. The difference in fat consumption will also be marked, but less so, and, as seen in Part III of this chapter, the difference here is largely due to a below-natural consumption in the East Pakistanis. Furthermore, any difference in fat consumption cannot explain a remarkable difference in the incidence of obesity in the two groups, which is so often associated with diabetes. For obesity is rare in the masses in East Pakistan, but extraordinarily common in the Cherokees. In the present conception the difference in sugar consumption explains the difference in incidence not only of the diabetes but also of the obesity.
Such, then, is the diabetes- and obesity-riddled state to which the spirited Red Indians of history and literature have been reduced by the exchange of a natural diet based on unaltered Indian corn (maize), plus game and fish, for the most unnatural alternative based largely on white flour and sugar.
d. Iceland
A little over a century ago proteins and fats were forming a high proportion of the diet of the Icelanders, and, as with the Eskimoes, diabetes was probably unknown. Thus, even in 1938 V. Jensson, Director of Public Health, stated: ‘Diabetes is a very rare disease in Iceland, and it is an extraordinary occurrence for doctors to come across it’ (quoted by Albertsson). [19]
Unfortunately, the present situation is very different. In 1850 proteins and fats formed 80-85 per cent of the national diet, [20] but with the replacement of these foods in later years by the refined carbohydrates (white flour and sugar) this figure was already reduced to 45 per cent in 1940, and today the sugar consumption in Iceland is that of the Westernized nations — well over 100 lb. per head per year.
With this change in the diet diabetes has first emerged and finally even become prominent. This development can be shown to have occurred within the 20-year incubation period worked out by G. D. Campbell, as already described.
There should be added to the foregoing, from Albertsson’s paper, that obesity, which was rarely seen in Iceland before the First World War, is now a common condition.
e. The Yemen
Perhaps the most striking of these aetiological studies, however, because of its thoroughness, has been A. M. Cohen’s (1960) upon the Yemeni or ‘Black Jews’. [21] These people moved to Israel from the Yemen, where they ate mainly fat and protein foods, and where their sugar intake was one of the lowest in the world. When they moved to Israel the most striking change in their diet was a marked increase in sugar consumption, and in a group of people in whom diabetes was unknown the incidence of the disease rose to that prevailing in Israel (which exceeds that in many Westernized countries). Similar findings were noted amongst Kurdish immigrants.
f. Islands in the Pacific
Similar evidence pointing to the consumption of refined carbohydrates in the aetiology of a rising incidence of diabetes is available from studies on the Australian aborigines; [22] on the primitive inhabitants of New Guinea; [23] and on the Polynesian inhabitants of Mabuig Island. [24] More recently this evidence has been extended for Polynesia. [25]
g. Westernized Nations
Turning now to the Westernized nations, we may say that sugar consumption is very high in all of them (e.g., England: 120 lb. per head per year, as shown in Chapter II), and that the incidence of diabetes is very high, too. Thus, the Birmingham Surveys on some 20,000 persons, whose ages approximated to the national average, showed an incidence of about 1 per cent of overt diabetes, and about another 5 per cent of latent diabetes (that is, where people have abnormal glucose-tolerance curves, or where they show these too readily under unfavourable conditions), in whom the conversion rate is expected to be high. The results of these surveys (which are still being followed up) were published in 1962 and 1963, [26, 27] and are not out of harmony with other, earlier surveys on white populations.
Owing to variations in the methods of blood-sugar testing, and especially owing to variations in the interpretations of results in these tests, it is not possible in a non-technical work like the present one to make a close comparison between these surveys and those in other racial studies, especially as the age structure, to which the incidence of diabetes is so closely linked, is often radically different, but it does seem that the Indians in Natal, and therefore potentially the Indians in India, are exceptionally vulnerable to the disease.
V. Hereditary Considerations in Diabetes
Since diabetes as a congenital abnormality virtually does not occur (and it will be shown shortly that even its occasional appearance in the first ten years of life does not invalidate this statement), and since in any case its incidence in many populations far exceeds the figure of 5 per 1000 which the author has already shown represents the upper limit of incidence in hereditary defects, he rejects unequivocally that diabetes is for practical purposes ever primarily caused by hereditary defect.
That there not uncommonly exists in people a personal make-up of the pancreas and related structures, which make-up is obviously hereditary and may have been magnified through an unfortunate marriage in the parents, and which now renders these people unduly vulnerable to a new factor in the environment, so that they acquire diabetes, is incontestable — but this is utterly distinct from hereditary defect, as already explained in Chapter I.
In the author’s opinion there is a grave danger at the present time, as pointed out in the earlier chapter, that the hereditary features in diabetes may distract attention from the external factor in the environment, which is the primary cause and the only thing that really matters. Apart from indicating the threat in certain types of marriage, and the need for special supervision in certain children (to shield them from the external factor), the attention should be riveted on the primary cause.
The report of the working party appointed by the College of General Practitioners [28] on the family history of diabetes seems to be entirely consistent with the view expressed above on the hereditary aspects of the disease. The more the genetic predisposing make-up becomes pronounced, the earlier the disease begins, in the presence of the external causative factor. Or, as stated in the summary of the report, ‘only diabetes of early onset has a strong genetic background’.
Diabetes in the First Years of Life
It is considered here that diabetes as a truly congenital complaint for practical purposes does not occur, even in the low ranges of incidence shown to hold for all congenital abnormalities, but that it does occasionally occur in the first years of life is incontestable. This fact is by no means in conflict with the present conception.
Thus G. B. Winter and others, [29] of the Department of Children’s Dentistry at the Eastman Dental Hospital, London, have recently shown that ‘there seems little doubt that in this country local factors are all-important in the causation of rampant caries in the deciduous dentition, and that the factor principally involved is the prolonged sucking of sweetened feeding bottles, hollow feeders and dummies’. Similarly, A. J. Salter [30] has drawn attention to the cariogenic effect of feeding infants, often from birth, on dried milks to which large amounts of sugar are added before or during reconstitution; and E. M. Sefton and J. Fletcher [31] to similar effects from using sweetened dummies. To the teat in these latter a small container is attached, of about 6-ml. capacity, to be filled with honey, treacle, syrups, etc., and ‘many cases have been recorded where, in association with such sweetened dummies, the teeth of children aged 9 months to 2 years have been totally destroyed in the course of a few months’. [32, 33] If these practices can materially affect the caries rate in the deciduous dentition, it is not hard to see that, in those rare cases where the pancreas is extremely vulnerable to the external factor, they can likewise produce diabetes.
Quite apart from the use of sweetened dummies, it is to be noted that cereals, usually sweetened, are nowadays commonly given even during the first few weeks of life. [34] It is also to be noted that when sugar is added to milk feeds it is nearly always sucrose that is added and not the natural milk sugar, lactose, which may also be of importance.
Owing to the wide-ranging nature of the present work, it is not possible here to distinguish other than quantitatively between juvenile and adult-onset diabetes. That is, from the aetiological point of view the two are assumed here to differ in degree, but not in kind, which also coincides with the author’s own beliefs in the matter.
References
1. Himsworth, H. P. (1949), Proc. R. Soc. Med., 42, 3 323.
2. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 42, No. 2, 55.
3. — (1962), Peptic Ulcer, 142. Bristol: Wright. (U.S.A.: Williams & Wilkins Co., Baltimore.)
4. Campbell, G. D. (1959), Congr. Abstr., S. Afr. Med. Ass., East London, 45. Cape Town: South African Medical Association.
5. — (1960), S. Afr. Med. J., 34, 332.
6. Joslin, E. P., Root, H. F., White, P., and Marble, A. (1959), The Treatment of Diabetes Mellitus, 10th ed. Philadelphia: Lea & Febiger.
7. Campbell, G. D. (1963), S. Afr. Med. J., 37, 1195.
8. Mitra, K. (1953), In Diet Surveys. Indian Council for Medical Research.
9. Walker, A. R. P., Holdsworth, C. M., and Walker, E. J. (1971), S. Afr. Med. J., 45, 516.
10. Berry, J. H. (1967), personal communication (8 May, 1967).
11. Seftel, H. C., Keeley, K. J., and Walker, A. R. P. (1963), S. Afr. Med. J., 37, 1213.
12. Jackson, W. P. U. (1963), Ibid., 37, 1220.
13. Banting, F. G. (1929), quoted by Campbell, G. D. (1966), Ibid., 40, No. 2, 21.
14. Poon-King, T., Henry, M. V., and Rampersad, F. (1968), Lancet, 1, 155.
15. Schaefer, O. (1971), Nutrition To-day, 6, No. 6, 8.
16. Bang, H. 0., Dyerberg, J., and Nielsen, A. B. (1971), Lancet, 1, 1143.
17. West, K. M., and Kalbfleisch, J. M. (1966), Diabetes, 15, 9.
18. Stein, J. R., West, K. M., Robby, J. M., Tirador, D. F., and McDonald, G. W. (1965), Archs. Intern. Med., 116, 842.
19. Albertsson, V. (1953), Diabetes, 2, 1184.
20. Steffensen, J. (1950), quoted by Albertsson, V., in reference 19.
21. Cohen, A. M. (1960), Israel Med. J., 19, 6137.
22. Cook, C. E. (1963), personal communication.
23. Campbell, C. H. (1963), personal communication.
24. Winterbottom, H. J. (1961), Med. J. Aust., 1, 780.
25. Prior, J. A. M., and Davidson, F. (1966), N. Z. Med. J., 65, 375.
26. College of General Practitioners (1962), Report of a Working Party appointed by, Brit. Med J., 1, 1498.
27. — (1963), Report of a Working Party appointed by, Ibid., 2, 655.
28. — (1965), Report of a Working Party appointed by, Ibid., 1, 960.
29. Winter, G. B., Hamilton, M. C., and James, P. M. C. (1966), Archs. Dis. Child., 41, 207.
30. Salter, A. J. (1965), Brit. Med. J., 1, 59.
31. Sefton, E. M., and Fletcher, J. (1962), Ibid., 2, 482.
32. Stephens, R. R. (1958), Practitioner, 180, 438.
33. James, P. M. C., and Parfitt, G. J. (1957), Brit. Dent. J., 103, 37.
34. Asher, P. (1968), Lancet, 1, 535.
Chapter VIII
Coronary Disease
‘Tu. ch’hai la bocca dolce …
Tu che il zucchero porti in mezzo al core …
(You, whose mouth is sweet …
And who instil sugar into the depths of the heart …)
— Serenade, Mozart’s ‘Don Giovanni’
THIS condition has been left till late, because the inclusion of coronary disease amongst the manifestations of the saccharine disease will be seen to depend rather on general reasoning than on specific reasoning. For with each of the other conditions studied hitherto the mechanism of production of the condition shows up quite clearly, but with coronary disease this is not the case. Therefore, reasoning of a more general order will be submitted on this occasion — which necessitates some consideration of the other conditions studied in this work.
It should be added that in these discussions it is accepted that differences in the pathology may reflect a rather different mechanism of production in the terminal thrombosis from that in the accompanying atherosclerosis, but as this is not a work on pathology such differences will not be pursued here, for that would interfere with the clarity of the general line of reasoning.
I. Coronary Disease, Human Evolution, and the Consumption of Fats
It will be advanced in this chapter that only an evolutionary approach to the tremendous and undiminished problem of the cause, prevention, and arrest of coronary disease is able to afford a solution sufficiently secure, and sufficiently quick, to be of any value to those alive at the moment. Prolonged investigations may help future generations, but not, it is submitted, our own. That the problem is a tremendous one is shown by the disease having now reached epidemic proportions, so that at present it accounts for a quarter of all deaths in the United Kingdom, [1] and in Scotland has become the commonest cause of death under the age of 35.
And that the problem remains undiminished is shown by the collective results of preventive dietary trials to date, which have centred on fat consumption, being essentially equivocal. [2, 3, 4] For example, the prolonged Framingham trial in the United States, that concerned itself mainly with fat consumption, has not achieved a convincing result, nor have similar trials in this country. A recently published trial in a mental hospital in Finland, [5] also interfering with fat consumption, does not, in the author’s opinion, surmount the criticisms passed upon it [6, 7] over coincident differences in sugar consumption (which consumption, it may be observed, was far above the natural [i.e., evolutionary] level). Indeed he, himself, would regard these results as not only not invalidating the arguments presented in this chapter, but also as unlikely to be considered in a free society as an adequate inducement to forgo natural tastes and pleasures in the eating of fats. These criticisms have very recently been added to by M. Halperin and others (Lancet, 1973, 2, 438, 439).
That the problem remains undiminished is also shown, it is submitted, by the sombre fact that our own profession suffers from coronary disease just as much as does the rest of the population, and quite possibly more so, to judge by the last figures available from Somerset House. [8]
In the following pages it must be taken as very clear that it is not in any way the author’s solution that is being put forward, but Nature’s own solution (to use again the convenient term, Nature, for evolutionary adaptation). And in this connexion it is suggested that right at the start there is borne in mind the wonders of the heart as a machine — a machine unparalleled, a machine whose action-cycle is repeated 100,000 times a day for 70 years, without a single refit or a single servicing. For a sense of wonderment is a valuable promoter of a sense of reverence, and without a sense of reverence for the body in general, and for the heart in particular, the following lines of reasoning can scarcely produce an impact on the mind of the reader.
From the above preliminary remarks it is beyond a doubt that the only chance of the heart preserving its structural integrity (that is, as a machine, continuing in serviceable repair) must lie in the meticulous maintenance of its natural environment — the environment achieved by evolutionary trial and error over many millions of years. And since the environment of the heart consists essentially of the blood-stream, and since the constitution of the blood-stream is basically dependent on the type of food eaten, it is above all on the naturalness of the food that the structural integrity of the heart must ultimately depend. Herein, it is submitted, lies the key to the solution of the coronary problem, and in the following pages, which are an expansion of a much earlier work of the author’s [9] on the same lines, it will be shown to what extent the evolutionary approach is being departed from, and even actively thwarted, today.
Evolution and Fat Consumption
The most glaring example of this departure from evolutionary principles is seen in the present-day interference with the fats in the diet, as already referred to. It is argued that because in coronary disease there tends to be an increase in some of the lipid, that is, fatty, components of the blood, such as cholesterol, and because this substance is also prominent in any atheromatous plaques that may be present, it is the fats in the diet that are in some way the cause of the trouble. Now, many consider that in coronary disease any pathological changes involving cholesterol are an associated, not a causative, event, similar to the deposition of cholesterol crystals in inflammations of the middle ear, but if cholesterol did play a causative role in coronary disease, would this be in conflict with the present conception, which will be seen shortly to involve the refined carbohydrates? The answer is no, for the following reason.
In the first place, cholesterol is not the only blood lipid that may be implicated in coronary disease. There are others, including the triglycerides, which are increasingly regarded as significant. [10] And though animal fats in the diet are well known to increase the blood lipids, sucrose in the diet is also becoming known to do this, especially as regards the triglycerides. A considerable and controversial literature, indeed, has accumulated on this latter point (involving sucrose and the triglycerides), I’ll but the truth is that the relationship of any one component in the diet to the blood lipids is liable to be controversial. [12] One reason for this lies in the difficulty over the controls, as set out in a later paragraph in this chapter. What is least controversial [12] is that any over-consumption of food and consequent energy imbalance, often leading to obesity, and to pre-diabetes and diabetes, is especially prominent in increasing the blood lipids, particularly the triglycerides. And it is here that the present conception enters the picture.
For the present conception holds, as seen in Chapters II and VI, that the absolutely dominant cause of over-consumption of food, itself leading to obesity and diabetes, lies in the concentration produced in the carbohydrates by refining processes. If in due course this contention becomes accepted — that in over-consumption Nature does not make a mistake, but is deceived in the sensations of hunger and satiety by the unnatural concentration present in products like sugar and white flour — then the refined carbohydrates will emerge as not only the dominant cause of over-consumption but also of an increasing rise in the blood lipids. And this regardless of the capricious and controversial results of individual tests involving fat, sugar, etc. Whether, as stated above, the increase in blood lipids is causative in coronary disease, or merely associated with it, will be referred to again later.
However, it is not with these biochemical trees that we are mainly concerned at the moment, but with the evolutionary wood. Those who incriminate animal fats in raising the blood lipids and causing coronary disease would have us stop eating the fats that we have been eating from immemorial time, such as the fat found in meat and in the butter and cream derived from milk, and eat instead a whole lot of new oils, mainly expressed from vegetable seeds, many of which oils are alien to us. The reason this substitution is recommended is because these oils contain greater amounts of polyunsaturated fatty acids, which when eaten increase the blood cholesterol little or not at all compared with their saturated analogues present in animal fats; and which are also considered to be more valuable to the body structurally. Indeed some, such as H. Malmros, [13] would have the above substitution carried out on a national scale, and in certain countries, like Australia, the very dairy industry has been threatened. Let us therefore look into this substitution more closely, from the evolutionary point of view, as suggested earlier by the author. [14, 15]
The keeping of flocks of sheep, herds of cattle, and other domestic animals, in order to provide a continuity of meat and milk, started with neolithic man many thousands of years before the Christian era, and even only 1500 years before that era Moses, in the Bible (Deuteronomy 32.14), was stating that Jehovah gave to his people to eat ‘butter of kine, and milk of sheep, with fat of lambs’. It is true that the consumption of fat in some parts of the Old Testament is forbidden, but this is always in connexion with the making of burnt offerings, the fat being needed for the performance of this act. It was once explained to the author by a guide of the great temple at Karnak in Egypt that every particle of these burnt offerings was eaten by the priests. And no one reading the first ten verses of the seventh chapter of Leviticus can doubt that the guide was right. To these ancient fats we are therefore well adapted, quite apart from man, as a hunter, being well acquainted with the fat of animals in evolutionary times far more remote than the neolithic ones.
Contrast with these ancient fats the new oils, mainly expressed from vegetable seeds. Not only are many of these seeds not a natural food for man (e.g., cotton seed and sunflower seed — and incidentally the sunflower does not even come from the Old World, as we do in the British Isles, but from the New), but also the oils expressed from many of them never existed in any quantity before the invention of the modern hydraulic press or the new solvent procedures, and consequently were scarcely eaten in this country before the introduction of margarine, circa 1916, during the First World War. Evolutionarily these oils make us not so much men as the equivalent of a flock of greenfinches, and the evolutionary incongruity is heightened by the fact that the coronary explosion amongst us, as will be seen later, came in since the introduction of just these oils at the period stated, though in margarine they are often saturated by a stream of hydrogen.
Evolution and Grass-fed Animals
At this stage we must digress to discuss an important point. Some have objected that the animal fats may be distorted by stall-feeding of the animals themselves. But even M. A. Crawford [16] has pointed out that the amount of polyunsaturated fatty acids in the fat of the domestic pig, which is perhaps the most stall-fed, as it were, of all the domestic animals, is some four times the amount in the fat of domestic cattle, largely fed on grass, and in the milk and butter obtained from cattle. However, let the battle be fought out where no stall-feeding is in question, as in the case of sheep. Not one of those who advise that animal fats be replaced by vegetable-seed and similar processed oils makes an exception over mutton fat, for this is a typical saturated fat. We are advised not to eat the mutton fat of grass-fed sheep, though we may love it. And this is the evolutionary crux — the thwarting of a natural taste for a natural food.
Indeed, an elaboration of this point arises here, for Crawford, [17] having been at great pains to demonstrate that domestic animals, like cattle and sheep fed on grass, have much more fat between the muscle fibres (‘marbling fat’) than in the case of their wild counterparts, has suggested that eating the meat of these grass-fed animals may hold dangers for us, since it may be akin to taking into the body pathological material, or ‘eating obesity’, as he has called it. But it is contended here that evolutionary considerations show this argument to be in serious error.
For though it is true that large numbers of domestic cattle (and still larger numbers of sheep, as already said) are fattened up for market in this country on grass, it would not be possible to fatten up wild cattle in this way, any more than it would be possible to fatten up a wild rabbit on grass as compared with the various breeds of hutch rabbit. No, it has taken very long periods of selective breeding to evolve animals that will behave in this manner. The situation is even better seen in the case of domestic ducks, most of which cannot fly off the ground. This is true, from the Aylesbury duck in this country to the flocks of domestic ducks seen along the rivers of China, each flock attended by a small boy. Thousands of years of selective breeding have been needed to replace muscle by fat to this extent (and the same period of time has been available for some adaptation in man to such food ). We must, therefore, very sharply distinguish this evolved fat (using ‘evolved’ in its transitive sense) from any fat that is remotely pathological. Else we shall be banning our best eating apples because they are so far removed from crab-apples, and our best wheat because it is so far removed from the primitive ancestral grasses. And it should be added that it is the above ‘marbling’ with fat that is partly responsible for the taste in lean meat; [18] without it there is a tendency for lean meat to have a watery taste.
Why do our tastes seek to increase the fat in animals and birds in the above manner (for who would compare the pleasure in eating most wild ducks with that in eating an Aylesbury duck)? The answer must surely be that, just as the body seeks in every posture, and in every activity, to economize muscular action, in order to minimize work on the heart, so also it seeks, by increasing in meat the ratio of fat — a food that is completely combusted — to minimize work on the kidney, an organ that plays so big a part, via the blood-pressure, in the length of life in each one of us. We should do well not to dismiss this frequent preference for fat from our reflections, which is present in perhaps a minority of people — but a very important minority.
But Crawford [16] attacks not only the quantity of fat, but also the quality, in grass-fed animals. He points out that the fat in domestic cattle is more saturated — i.e. has a higher ratio of saturated fatty acids — than occurs in the fat in wild African cattle feeding on a more varied diet. Yet his list of wild animals includes the Uganda kob, of the plains, with the identical fatty acid ratios present in our own cattle and in the milk and butter obtained from them. Is it to be supposed that we should come to harm, especially coronary harm, if we often ate the African kob?
Furthermore, nearly all the fat we eat is combusted for heat, only a small part being retained for structural replacement. Why should not the body combust the fat that is less valuable and retain for replacement the fat that is more valuable, just as it does so miraculously with other foods? How quickly do scurvy and other deficiency diseases disappear directly the missing substances appear in the diet!
It may well be, in fact, that sometimes the body may prefer a high ratio of saturated, combustible fat. It will be recalled that only some 67 years ago Metchnikoff, [19] Director of the Pasteur Institute, in his Prolongation of Life directed the attention of all Europe to the longevity of certain Bulgarian peasants living on milk and milk products — which abound in saturated fats. The influence of this work is still with us today, as seen in the common taking of yoghurt, and stands as a perpetual challenge to those who would have us depart from eating natural foods, naturally desired.
Far from indicating, therefore, that the substitution of unsaturated vegetable and other oils for saturated animal fats has any value in the prevention and arrest of coronary disease, the evolutionary approach points to the exact opposite — and in addition points to the following danger. For, as touched on above, it was not until the invention of the modern hydraulic press, or the new solvent procedures, that cotton-seed oil and some other processed oils ever appeared in any quantity on the surface of this planet. With the exception of olive oil, few of them, as already stated, were eaten at all before the First World War. The question, therefore, arises as to whether the consumption in large amounts of substances that are essentially alien to the human body carries any risk with it — especially the risk of cancer, which always tends to be related to substances foreign to the natural environment. This risk would certainly not be lessened by the passing of a saturating stream of hydrogen through some of these processed oils, in the interests of achieving a greater solidity for table use, as in margarine.
It may therefore be no coincidence that in a recent dietary trial in the United States, [20] involving just the substitution in fats now under consideration, there appeared an undue occurrence of cancer cases. Years of observation, or careful animal experiments (of which the results to date are not wholly reassuring [21] ), may or may not throw further light on this event, but what is important is the principle involved. It is submitted that no one who has any reverence for the human body, as set out at the beginning of this chapter, will ever choose to substitute these new processed oils for animal fats of ancient lineage. What economic forces dictate, alas!, is another matter.
Before concluding this part of the present chapter the author would add that he, himself, no longer attaches much importance to the condition of essential (familial) hypercholesteraemia in the search for the causation of acquired coronary disease. He considers the element of hereditary defect in this complaint is too great for it to be of very much value in this respect, involving as it does the metabolism of cholesterol itself, which need be no more related to the deposition of cholesterol in the atherosclerosis of higher age groups than congenital flat foot is related to acquired flat foot. Furthermore, some of the types of essential hypercholesteraemia distinguished by D. S. Frederickson [22] appear to be verging on the acquired type (and it is worth remembering that no known hereditary defect, as seen in Chapter I, occurs more often than five times per 1000 live births), with carbohydrate consumption often strongly implicated. But this rare and complicated disorder cannot be discussed at length in a wide-ranging work of the present type.
Finally, in the previous evolutionary study already mentioned, the author advanced that if fat consumption played any part in the causation of coronary disease, it did so via the agency of arbitrary food mixtures, as set out in Chapter X, Section IX. These include fried foods, where people may have to eat fat they do not want in order to eat meat, fish, or eggs they do want; or such foods as chocolate or ice-cream, where unwanted fat may be eaten for the sake of the accompanying sugar. (The vast increase in ice-cream consumption is shown in the accompanying table.) A causative fat consumption of this type, which, as was explained, is not seen in Nature, would never be in conflict with human evolution, and the value of avoiding these mixtures as much as possible in any system of natural nutrition is referred to in the diet card at the end of this volume. (But the application is not especially to coronary disease; it is also applicable to such conditions as peptic ulcer and the dyspepsias.)
Thus ice-cream, previously alluded to, shows the following increased consumption in the British Isles during the period stated, in thousands of gallons:
| 1920 | 1930 | 1938 | 1951 |
| 870 | 7890 | 35,607 | 39,612 |
| Board of Trade (1951) ‘Report on the Census of Production for 1951. Ice-cream’. London: H.M.S.O. | |||
Not only is the study of this unnatural type of fat consumption neglected at present, but in the author’s opinion the study of other, allied aspects of fat consumption is also neglected. These aspects concern the markedly different personal inclinations that exist over fat consumption, so that some people, like Jack Sprat, desire very little fat, whilst others, like Mrs. Sprat, desire a great deal of it. These striking personal differences are of evolutionary origin, as set out by the author in his earlier work. For in man a higher proportion of calorific needs is derived from fat in cold climates than it is in hot climates. Even in Europe some 40 per cent of the calories are derived from fat in northern parts, as against some 20 per cent in southern parts, like the south of Spain and the south of Italy. [23] Thus in Great Britain, where the population is of mixed descent, due to past invasions from the north and south of Europe, and in the United States, where the white population is also of heterogeneous descent, both Jack Sprats and their opposites abound. Consequently in some people a low fat consumption, when evolutionarily considered (that is, in terms of natural tastes), may be too high, whilst in other people a high fat consumption may, similarly, be too low. Such departures from the natural level may be due to financial or other factors, including mass feeding in schools and institutions.
Clearly any attempt to relate fat consumption to coronary disease would have to take into consideration not only the above evolutionary differences, but preferably also any marked departure from these differences, due to the external factors mentioned. Yet there is little or no evidence of such consideration and we find bold comparisons being made between, for example, fat consumption in the Danes and in the African Bantu. [23] More particularly, those who contest the relationship of refined carbohydrates to coronary disease, and especially those who contest certain clinical studies relating personal sugar consumption to the disease, forget that clinical studies [24, 25] have never demonstrated any relationship whatever between personal fat consumption and the disease.
With these points very much in mind we now proceed to the second part of this chapter, where the historical and epidemiological aspects of fat consumption will be discussed with the refined carbohydrates.
II Coronary Disease, Human Evolution, and the Consumption of Refined Carbohydrates
In the second part of this chapter there will be brought forward evidence relating coronary disease to the consumption of refined carbohydrates, and for including it in the saccharine disease. This evidence will be presented under evolutionary, historical, and epidemiological aspects.
Evolutionary Aspect
In contrast with the evolutionary incompatibility in relating coronary disease to the consumption of animal fats, as set out above, the relating of the disease to the consumption of refined carbohydrates presents no incompatibility whatever. For in the latter case the disease is being related, not to ancient and natural products, to which we are now well adapted, but to new and unnatural products, to which we can hardly be adapted at all. This aspect will be further elaborated in some of the following paragraphs.
Historical Aspect
The new event of the refining of carbohydrates, as exemplified in the production of white flour and commercial sugar, has already been described in Chapter II, together with the relevant dates of the period concerned, and to that chapter, in order to avoid repetition, the reader is now referred. For the reasons carefully given in that chapter there has been little increase in fat consumption during a similar period of time. Indeed, two of the four references that were cited, M. A. Antar, M. A. Ohlson and R. E. Hodges, as also B. Friend, showed not only that total fat consumption in the United States increased by only 12 per cent over a recent 70-year period, but also that such increase took place chiefly in the consumption of just those processed vegetable and other oils that were seen in Part I often to be recommended in the prevention of coronary disease today.
In contrast with this small increase in fat consumption, the increase in sugar consumption, over the period shown in the chart in Chapter II, has been no less than sevenfold, and although the consumption of white flour, which was pointed out as already widespread at the beginning of the period (circa 1800), has fallen somewhat during the later part of the period, this affords no consolation, for, as was also pointed out, such fall has been due to the greater, and more dangerous, consumption of the still more refined carbohydrate, ordinary sugar.
Meanwhile, as regards coronary disease itself, and more particularly coronary thrombosis, the main explosion in the incidence has by common consent occurred since 1900, and especially since 1920. [1] A. Keys has recently argued that this is too long after the main rise in sugar consumption for the disease to be related to this consumption. But in his paper Keys makes no reference to the all-important incubation period. Indeed, in by-passing this aspect of the problem, his argument appears to become meaningless. For the incubation period in diabetes has already been shown to average some 20 years, and since over 50 per cent of maturity-onset diabetics die of coronary disease, and since, also, the latter disease is seldom seen under the age of 30, we must regard 30 years as the minimum incubation period in most cases of the disease — and it may be very much longer. This 30-year minimum incubation period, which points to the fuse as it were, of the beginning of the coronary explosion being lit around the year 1890, when sugar consumption was rapidly approaching the 100-lb. mark, is just as vital in seeking the cause of coronary disease as, for example, the 40-year incubation period is in seeking the cause of diverticular disease. No comparable fuse is to be seen in fat consumption. Indeed, a review of dietary changes in Britain [26] points to the consumption of dairy produce and fats having increased mainly in the 1930s — ‘some time after, and certainly not before the start of the coronary epidemic’. [1]
Epidemiological Aspect
1. The Clinical Association of Coronary Disease with Diabetes and with Obesity
In coronary disease far and away the most important epidemiological fact (to record it under this heading) is considered here to be the association of the disease with diabetes, which is well accepted. (Though diabetes itself is strongly associated with obesity, the association of coronary disease with obesity is somewhat more complicated, so we shall mainly confine ourselves here to the association with diabetes.) If, now, the causation of diabetes (and, for that matter, of obesity) lies essentially in the consumption of refined carbohydrates, as contended in Chapters VII and VI, then the argument for coronary disease having the same basic causation becomes strong indeed. Meanwhile, such crucial association cannot be explained in terms of fat consumption. This is seen in Chapter VII as regards diabetes; and as regards obesity, a high-fat diet has actually been used as a reducing diet. [27]
The key value of the clinical association of coronary disease with diabetes, in the elucidation of the cause of coronary disease itself, is shown in the following examples. Thus, when again remembering the 100,000 beats of the heart each day, one is ever amazed that, amongst other things, the endothelial lining of the coronary artery is able, in the midst of such gross physical turmoil, to maintain its integrity — especially as the least impairment of that integrity, the least injury (e.g. of a ‘crinkling’ nature, as it were) to that endothelial lining, would initiate a deposition of clot, and from that a possible thrombosis of the artery. Now since the C vitamin is well known to be one of the food substances most intimately concerned in the nutrition of the endothelial lining of arteries (and hence the widespread escape of blood from the small vessels in scurvy, where this vitamin is lacking), it would seem a plausible hypothesis that coronary thrombosis should reflect the known and frequent deficiency of this vitamin in the food of Westernized peoples today, through its effect on the nutrition of the endothelium, especially at the points of greatest strain. G. F. Taylor [28] has shown how real is the present lack of vitamin C, especially in older people, but such lack cannot be the basic cause of coronary thrombosis, for it cannot explain the association of the disease with diabetes. That a lack of vitamin C could be an aggravating factor in coronary disease, yes, but the basic cause, no. And exactly the same argument will be seen later to apply to smoking; a powerful aggravating factor, yes, but the basic cause, no.
At this point it is desirable to reflect on the distinction between the basic cause of a condition and multiple aggravating factors. For unless such distinction is carefully preserved, the very unhelpful phrase ‘of multifactorial origin’ is liable to be used, especially in connexion with coronary disease. Not only does such a phrase, in the author’s opinion, usually not reflect clear thinking, but it also has the serious objection of interfering with the attack on the causative factors in order of their importance. The distinction is well seen in the case of tuberculosis. [29] This disease, also, was once thought to be of multifactorial origin, because of the accompaniments of under-nutrition, overcrowding, heredity, and other factors. But directly the tubercle bacillus was discovered, this diffuse aetiology was replaced by a single basic cause and multiple aggravating factors — and a big step forwards in prevention became possible. For the removal of aggravating factors merely dents the incidence, whereas the removal of the basic cause reduces the incidence to zero. And in this lies the true importance of the distinction.
With further reference, now, to the clinical association between coronary disease and diabetes, since it is considered here that both conditions arise from a common cause (the consumption of refined carbohydrates), and not that one of these conditions arises from the other, it follows that either condition may be the first to arise, depending on the personal make-up in the person concerned, though usually it is the diabetes that appears the first. In this connexion the author wishes to refer to the illuminating studies of Professor H. Keen and others, [30, 31, 32] who have shown that people with high blood-sugar curves (the forerunner of overt diabetes) have a much higher incidence of coronary disease than those without this sign. These studies, which are of several years’ duration and still continuing, are in close accord with others in Tecumseh, U.S.A., in Paris, and in Australia. Unfortunately space precludes their pursuit here, but they are lucidly set out in the references given and their importance to the present argument is clear. The subject has been well summarized by F. H. Epstein. [33]
From this work it is also clear that a persuasively simple mechanism might be concerned in the production of coronary thrombosis, which is more direct than one centred on the blood lipids, previously mentioned, though it must be repeated that the latter is by no means incompatible with the present conception, as will be enlarged on shortly.
For an unnaturally high blood-sugar, constantly impinging on the endothelial lining of the arteries, over many years, might cause degenerative changes in this endothelium, and, by diffusion, in the arterial wall, too, especially at the sites of greatest strain (of which the commencing aorta and the coronary arteries are the supreme examples). This degeneration could then initiate the thrombosis which so often brings the sequence to a close. Such a sequence, indeed, involving the conversion of glucose into non-diffusible sorbitol in the arterial wall, is under present investigation. [34]
The high blood-sugar in such a mechanism would stem primarily from a concentrated (refined) diet, any pancreatic exhaustion from the same cause then raising the blood-sugar still higher. Whether such pancreatic exhaustion, raising the blood-sugar still higher, proceeded to overt diabetes before, or after, the endothelial degeneration reached the critical stage of producing’ a (coronary) thrombosis would depend on the personal make-up in the individual concerned, but usually the diabetes appears the earlier, as already said.
In connexion with the above mechanism a recent paper by S. Wapnick [35] and others becomes of great importance, for these workers, who studied 50 poor Africans, 35 African medical students, and 12 Europeans, with increasing Westernization of the diet accompanying the higher economic status in each of the three groups, showed how closely the consumption of sugar and white flour affected the fasting and active blood-sugar levels. Thus the natural blood-sugar levels are probably as different from the ‘normal’ levels in people on a Westernized diet as the natural transit times of the intestinal contents have been shown to be different from the ‘normal’ transit times in people on this diet, too (Chapter III). And just as the difference in transit times gives the vital clue to the causation of diverticular disease, so it is contended here may the difference in blood-sugar levels give the vital clue to the causation of coronary disease.
Though it would probably take years to prove, or disprove, that the above mechanism does lie at the centre of the many collateral changes that take place in coronary thrombosis, at least the suggested sequence gives an immediate guide to natural prevention, as set out at the end of this work.
Meanwhile, it must be repeated that the fall in the glucose tolerance and the rise in the blood-sugar, which are both so characteristic of pre-diabetes and diabetes itself, are accompanied by striking increases in some of the blood lipids, especially the triglycerides. Hence if it is preferred to relate coronary disease to changes in the blood lipids, rather than to changes in the blood-sugar, it is still not difficult to involve the refined carbohydrates in the former changes. Of one thing the author is very confident; the key to causation of coronary thrombosis lies in the causation of diabetes (and also of obesity ).
2. Racial Studies
In the search for the causation of coronary disease, important racial evidence has been advanced from South Africa. In the first place there has been the almost complete freedom from coronary disease in Africans living tribally on unrefined carbohydrates, which is generally recognized. Typical of these Africans are the members of the Zulu tribe described in certain chapters of this work, especially in Chapter VII, where the rarity of diabetes in them has also been stressed. This freedom from coronary disease is, however, gradually being lost in urban Africans, on a more Western diet, with much refined carbohydrate. However, this change is far better seen in their cousins, the Negroes in the United States, where, in comparable occupations, the incidence of the disease, like the incidence of diabetes, is not greatly different from that in the whites, [36] just as their consumption of refined carbohydrates is not either. I am privileged to quote the following personal communication from G. E. Burch of Tulane University, New Orleans, to Mr. Denis Burkitt, F.R.S., 13 July, 1971: ‘Concerning the incidence of coronary disease among the Negroes, it is true that the incidence was extremely low among Negroes, and practically non-existent among the Negro females, many years ago. At the present time, however, the incidence is essentially the same as in the whites… There is no doubt that the incidence has increased considerably in the past ten years.’
Turning now, in the second place, to the Natal Indians, their case is even more instructive. This is partly because their exceptionally high incidence of diabetes, described in Chapter VII, is matched by an exceptionally high incidence of coronary disease also; and partly because, as set out in the earlier chapter, their high consumption of sugar and other refined carbohydrates contrasts with a fat consumption where the animal fats are far less in evidence than the processed vegetable oils. Consequently, as regards coronary disease, the fat consumption in these Indians may well be as illuminating as their sugar consumption. Meanwhile it is generally recognized that in India itself, where sugar consumption has already been shown to be extremely low, coronary disease is relatively inconspicuous, except amongst the upper strata of society, where the food structure often resembles that in Westernized countries.
But what is of particular importance to the present work is that S. L. Malhotra [37] has shown that the incidence of the disease is seven times commoner in the south of India than it is in the north. For in the south the diet is largely refined rice, with only 31 per cent of the calories supplied by fat (and largely seed oils at that), whereas in the north the diet is largely unrefined wheat and maize, with no less than 23 per cent of the calories supplied by fat (and largely animal fats at that). Indeed, the polyunsaturated fats constitute 45 per cent of the fats in the south but only 2 per cent of the fats in the north (Indian Council of Medical Research). [38] Yet, as stated, coronary disease is much commoner in the south.
At this point it must be interjected that Malhotra has performed these geographical studies in India on railway workers, so as to eliminate socio-economic and certain other factors as much as possible, since the north of India is often economically better off than the south. This makes it easier to compare staple dietetic differences between the two parts.
It is true that sugar consumption is lower, not higher, in the south, but, as has been stressed in the case of diabetes (Chapter VII), it is the consumption of all types of refined carbohydrates that is important, not only that of sugar, and in this respect the south of India, with its predominant diet of white rice, easily leads the north. It is worth noting, too, that as regards the conception of the saccharine disease, the same southern part of India, where coronary disease is relatively common, is just the part where peptic ulcer is also common (see Chapter X).
While Malhotra in his paper states that the seven times greater incidence of coronary disease in the south of India, in spite of the nine times greater consumption of fat in the north, does not support the view that coronary disease is related to fat consumption, including the saturation present in the fat, he appears to the author to miss the point when he says that the epidemiological picture does not support the view that the disease is related to sugar consumption, either. It is submitted that if Malhotra had regarded the consumption of all refined carbohydrates, he would have perceived a very accurate correlation indeed, and need not then have sought out a complicated aetiology based on local cooking patterns, which would seem to have little application in other parts of the globe. But his references to dietary fibre strongly support the present conception, as this has already been shown to decide the crucial question of over-consumption.
However, lack of fibre cannot be the direct cause of coronary disease, since that would make the clinical associations all wrong, set out in Chapter II. That is to say, it would cause the disease to be most associated with conditions directly due to loss of fibre, such as constipation, haemorrhoids, varicose veins, and diverticulosis, instead of, as it is, with conditions due to over-consumption, such as diabetes, obesity, and gall-stones. This is set out in Chapter II, and has a vital bearing on prevention and treatment, as also set out there. For if the cause lay directly in loss of fibre, the treatment would consist in the giving of bran, instead of, as it should, mainly in the replacement of sugar consumption.
At this stage a further reference must be made to the Yemeni or ‘Black Jews’, referred to in Chapter VII, in whom A. M. Cohen [39] and others have shown that coronary disease, no less than diabetes, has dramatically increased during 25 years’ residence in Israel, where by far the biggest change in the diet has been in sugar consumption, with relatively little change in fat consumption.
Finally, other primitive peoples than the tribal Africans described above could be referred to, such as the Polynesians. [40] None, whose food structure still continues at the evolutionary level, have been found to suffer from coronary disease, but only the Eskimoes and the Masai tribe in South Africa can be given space here. Both these peoples pursue a highly carnivorous existence, with an abundant consumption of meat and fat, which latter in the Masai includes large quantities of milk. [41] If the freedom from coronary disease in these two peoples is advanced as fatal to the fat-consumption cause, it is countered by the holders of that view with two arguments that are gravely weakened by their total dissimilarity — that the fats eaten by the Eskimoes are unsaturated compared with our own animal fats, and that the Masai, in their metabolism, have learnt to accommodate the saturated fats eaten by them, by suppressing their own cholesterol synthesis. [41]
Expressed in evolutionary terms, however, it cannot be concealed that those advancing these arguments allow the Eskimoes and Masai to eat the fats they are evolved to, but do not allow us to eat the fats that we are evolved to, such as the fat of lambs fed on grass, which, as was realized even by the priests of thousands of years ago, is when roasted so delicious.
3. The Importance of Considering All Forms of Refined-carbohydrate Consumption
This importance has been stressed in Chapter VII, in connexion with diabetes (Chapter VII), and in the earlier paragraphs of the present chapter, but the time has now come to look into this matter more closely.
Let us suppose that some investigator was engaged in a project, which at first sight would seem a sitting target, to relate obesity to the consumption of sugar. Surprisingly, someone opposing such a relationship would have no trouble at all in turning the tables on the investigator, for he would be able to assemble a collection of the fattest men in any town, who did not have a sweet tooth between them and in consequence consumed very little sugar at all. These people would represent the formidable army of beer-drinkers in this country — people who, in their tastes, prefer the bitter to the sweet. [42] And the reason the beer often causes extreme obesity lies not in its content of alcohol (which substance, of itself, when taken to excess, causes wasting), but in its content of malt sugar. Indeed, through the presence of this malt sugar (which is not a sweet sugar), beer becomes a perfect example of a refined carbohydrate. This case, like the case of diabetes in Trinidad (Chapter VII), shows the importance of relating any manifestation of the saccharine disease to the consumption of all forms of refined carbohydrates and not only to one form. For all of them end up substantially as glucose in the blood, as noted in Chapter II.
This crucial point, in the author’s opinion, partly explains why J. Yudkin’s findings of a high sugar consumption in coronary sufferers has not been confirmed by other investigators and in particular by a Medical Research Council working party. [43]
The same point can be used against the paper by A. Keys, [11] previously referred to, who found that certain countries having a higher sugar consumption had a lower incidence of coronary disease, for no refined carbohydrates, e.g. malted liquors, other than sugar were ever taken into account. Furthermore, Keys did not distinguish, in countries like Cuba, between natural sugar consumption, as in chewing sugar-cane, and unnatural sugar consumption, as in eating the refined sugar of Westernized countries today. The vital difference between these two types of consumption has been set out in Chapter II. And, lastly, the ignoring by Keys of the equally vital incubation period in coronary disease has already been referred to. His countries having a high sugar consumption, but a low incidence of the disease now, may well be heading for a very high incidence indeed — just as Great Britain was doing around the year 1890.
4. The Nature of the Controls used in Some of these Investigations Today
A further point must now be raised in connexion with many investigations today relating coronary disease to the consumption of refined sugar, or denying such relationship. This concerns the nature of the controls.
Consider once more the case of hallux valgus discussed in Chapter I. In this condition the basic cause was held to be the new environmental factor of wearing shoes (new, because the majority of mankind still go barefoot even today). But, as was shown, the factor of personal make-up also comes into the picture, because the make-up of certain feet, which are entirely free from any hereditary defect, may render these feet unduly vulnerable to the new factor now under consideration. Consequently, if an investigation of hallux valgus were made in those who wear shoes and those who do not, the basic cause would be starkly revealed; but if, instead, an investigation were made in subjects all of whom wear shoes, to see if the condition were related to narrowness in the shoe, such cause might not by any means be easily revealed. Some subjects with a high degree of vulnerability might have hallux valgus with shoes showing little narrowness, [44] and vice versa. Very large numbers of subjects might have to be investigated to establish the cause in this way.
And so it is with coronary disease and sugar consumption. It is far easier to establish the truth by investigations contrasting those who get much coronary disease and consume much sugar with those who get no coronary disease and consume no sugar either (as has, for practical purposes, been the case until recently with the tribal Africans described in this work) than by investigations of coronary disease and sugar consumption in those who all belong to a high-sugar-consuming community.
Directly following the publication of the author’s letters in The Lancet [45, 46] on these lines there appeared, by a remarkable coincidence, a paper in the British Medical Journal describing an actual investigation on hallux valgus, in St. Helena, by I. B. Shine, [47] which corroborated in practice every detail of the above argument.
The same argument has been very well summarized by D. Jennings: [48] ‘If everyone smoked 30-60 cigarettes a day, I doubt if even Doctor Richard Doll would have had the patience to compile the enormous statistics needed to show that 50-60 cigarettes a day were more damaging than 30-40.’
5. Smoking and Coronary Disease
Whilst fully persuaded of the importance of smoking in the aetiology of coronary disease, possibly through its constricting the terminal arterioles, the author is convinced that smoking constitutes an aggravating factor and not a basic cause. The main reasons for his conviction lie in the fact that though there is still a very considerable incidence of the disease in non-smokers, there is no incidence at all in primitive societies (such as the tribal Africans dealt with in this work). In short, the tubercle-bacillus argument used above is considered to apply very much here, too. Furthermore, smoking cannot explain the crucial association of coronary disease with diabetes. There are also historical considerations, as summarized by L. Michaels. [49]
In connexion with smoking, a further comment is indicated on the report of the M.R.C. Working Party mentioned earlier. This study referred only to the consumption of sugar and not to the consumption of all refined carbohydrates, and the controls were all from a high-sugar-consuming population, on the lines set out above. The report is not, therefore, considered to constitute a threat to the present conception. [50] The report associated coronary disease with the smoking of cigarettes, induced by the taking of hot sweet drinks, rather than with the consumption of sugar, but the present author has suggested [42] that if the consumption of other refined carbohydrates — especially beer — had been added to the consumption of sugar, exactly the opposite conclusion would have emerged. The report itself shows how marked is the association between smoking and alcohol consumption.
6. Exercise and ‘Stress’
It is not possible to conclude this chapter without some consideration of exercise and of ‘stress’, since a deficiency of the former, or an excess of the latter, is so frequently blamed for coronary disease today. As already set out in Chapter VI and Chapter X, the blaming of either of these factors is not remotely compatible with human evolution, especially as neither factor is ever considered in association with natural desires in these matters. For with regard to exercise, evolved sensations tend always to keep physical exertion in any pastime to the agreeable minimum, in order to reduce wear and tear of the body in general and of the heart in particular; and with regard to stress, the very mainspring of evolution has always consisted of the struggle for existence, where the killing of one organism by another represents stress in its starkest form. If we are adapted to anything in this world, we are certainly adapted to stress. To advise someone, who wants to rest, to take exercise is as unnatural as to advise someone, who wants to throw himself into the fight and get on in the world, to moderate his effort. Furthermore, this latter advice, applied to a whole country, would inevitably lead to national decline.
This is not to say that worry — another and serious example of stress — is desirable. It is very undesirable, but it is implicit in the struggle for existence, representing part of the mental effort in that struggle, and though it may cause loss of appetite and weight, it will not — in the properly nourished body — cause organic disease.
Since this book is based on natural, that is to say, evolutionary, principles, the author does not propose to pursue these two suggested causes of coronary disease any further. Neither of them can explain the crucial association of the disease with diabetes. And to allude to epidemiological details, such as the longevity attributed to hermits, who take little exercise, and to the longevity certainly occurring in many zoo animals, who take even less, would savour to him of setting out to prove an evolutionary axiom. Suffice it to say that, in the author’s opinion, trying to be clever at Nature’s expense, so well seen in combating the above two suggested causes of coronary disease, is the exact reason why, in spite of all the expenditure of money, time, and energy, so little has been achieved in the prevention of the disease to date. In particular, the countering of excess consumption, arising from the eating of refined carbohydrates, by the taking of unwanted exercise is considered a perfect example of two wrongs not making a right, even though the extra exercise is well known to reduce the consequences of such over-consumption.
Conclusion
The author would like to end this chapter with a quotation from the earlier joint work, with which A. Keys [11] ended his own paper, alluded to above:
‘But the propaganda keeps on reverberating and is reflected in such statements as the following: “We ourselves are confident that if the refined carbohydrates were avoided by reducing the diet to the practical evolutionary level we have set out, the incidence of coronary disease would in due course be reduced to almost nil”.’ [51] But Keys refrained from giving the vital end of this sentence, which ran: ‘as indeed it actually is in those communities, like the tribal Zulus in Natal, where carbohydrates until recently have been at this evolutionary level’.
The present author composed that sentence and he repeats it here. Nor is it always necessary to study such primitive peoples as these. Even amongst advanced countries, anyone who is aware of the difference between the food seen in France, often still consisting of natural materials, and the food seen in Britain — for example, in a great city like Glasgow — often consisting of tinned or refined materials, quite apart from a much smaller sugar consumption in France and much beer drinking replaced by wine drinking, will have little difficulty in understanding the striking difference in coronary mortality in the two countries, with France having about the lowest, and Britain (especially Scotland) about the highest, in Europe. [52]
To sum up, the author believes that solely by close attention to evolutionary principles can we hope to escape the coronary danger menacing each one of us today. This naturalness, and the simplicity in reasoning referred to in the Preface, have been the two objectives that he has tried specifically to pursue in the present chapter.
References
1. Meade, T. W., and Chakrabarti, R. (1972), Lancet, 2, 913.
2. Medical Research Council (1965), Ibid., 2, 501.
3. Medical Research Council Report (1968), Ibid., 2, 693.
4. Leader (1968), Ibid., 2, 901.
5. Miettinen, M., and others (1972a), Ibid., 2, 835.
6. — (1972b), Ibid., 2, 1418
7. Yudkin, J., and Rivers, J. (1972), Ibid., 2, 1026.
8. Population Censuses and Surveys. Data for 1961. London: H.M.S.O.
9. Cleave, T. L. (1957), Fat Consumption and Coronary Disease. Bristol: Wright.
10. Carlson, L. A., and Bottiger, L. B. (1972), Lancet, 1, 865.
11. Keys, A. (1971) Atherosclerosis, 14, 193.
12. Kannel, W. B. (1971), Nutrition Today, 6, No. 3, 2.
13. Malmros, H. (1969), Lancet, 2, 479.
14. Cleave, T. L. (1969), Ibid., 2, 600.
15. — (1969), Ibid., 2, 961.
16. Crawford, M. A. (1968), Ibid., 1, 1329.
17. — (1969), Ibid., 2, 1419.
18. Commonwealth Bureau of Animal Nutrition, Aberdeen (1970), personal communications from D. L. Duncan, Director.
19. Metchnikoff, E. (1907), Prolongation of Life. London: Heinemann.
20. Pearce, M. L., and Dayton, S. (1970), Lancet, 1, 464.
21. Carroll, K. K., and Khor, H. T. (1971), Lipids, 6, No. 6, 415.
22. Frederickson, D. S., and Levy, R. I. (1972), ‘Familial Hyperlipoproteinaemia’, in The Metabolic Basis of Inherited Disease, 3rd ed. (edited by Stanbury, J. B., Wyngaarden, J. B., and Frederickson, D. S.), 545. New York: McGraw-Hill.
23. Keys, A. (1955), in National Research Council, Washington, Symposium on Atherosclerosis, 187 and 238.
24. Paul, O., Lepper, M. H., Phelan, W. H., Dupertuis, G. W., MacMillan, A., McKean, H., and Park, H. (1963), Circulation, 28, 20.
25. Kannel, W. B., and Gordon, T. (1970), The Framingham Study, Section 24. National Institute of Health, U.S. Dept. of Health, Education and Welfare.
26. Greaves, J. P., and Hollingsworth, D. F. (1966), World Rev. Nutr. Diet., 6, 34.
27. Kerwick, A., and Pawan, G. L. S. (1956), Lancet, 2, 155,
28. Taylor, G. F. (1972), J. Inst. Public Health Hygiene, 3, 244.
29. Fowler, P. B. S. (1968), Brit. Med. J., 4, 57.
30. Boyns, D. R., Crossley, J. N., Abrams, M. E., Jarrett, R. J., and Keen, H. (1969), Ibid., 1, 595.
31. Abrams, M. E., Jarrett, R. J., Keen, H., Boyns, D. R., and Crossley, J. N. (1969), Ibid., 1, 599
32. Keen, H. (1971), Acta Diabetologica Latina, vol. VIII, Supplement 1.
33. Epstein, F. H. (1967), Circulation, 36, 609.
34. Morrison, A. D., Clements, R. S., and Winegrad, A. I. (1970) Atherosclerosis (ed. by Jones, R. J.). New York: Springer-Verlag.
35. Wapnick, S., Wicks, A. C. B., Kanegoni, E., and Jones, J. J. (1972), Lancet, 2, 300.
36. Cassel, J. C. (1971), Arch. Intern. Med., 128, 887.
37. Malhotra, S. L. M. (1967), Brit. Heart J., 29, 337.
38. Indian Council of Medical Research (1963), Spec. Rep. Ser., No. 42, 141.
39. Cohen, A. M., Bavly S., and Poznanski, R. (1961), Lancet, 2, 1399.
40. Hunter, J. D. (1962), Federation Proceedings (1962), 21, Suppl. No. 11, 36.
41. Bliss, K., and others, quoted in Shafer, A. G. (1972), Brit. Med. J., 4, 32.
42. Cleave, T. L. (1971), Lancet, 1, 43
43. Bennet, A. E., Doll, R., and Howell, R. W. (1970), Ibid., 1, 1012.
44. Haines, R. W., and McDougall, A. (1954), Ibid., 2, 1308.
45. Cleave, T. L. (1965), Ibid., 1, 1069.
46. — (1965), Ibid., 1, 1331.
47. Shine, I. B. (1965), Brit. Med. J., 1, 1648.
48. Jennings, D. (1968), Lancet, 2, 1249.
49. Michaels L. (1966), Brit. Heart J., 28, 258.
50. Heaton, K. W. (1971), Lancet, 1, 185.
51. Cleave, T. L., Campbell, G. D., and Painter, N. S. (1969), Diabetes, Coronary Thrombosis and the Saccharine Disease, 2nd ed. Bristol: Wright.
52. (1968) United Nations Statistical Yearbook, and World Health Statistics Annual.
Chapter IX
Primary Escherichia coli Infections and Other Conditions
I. Primary Escherichia Coli Infections
AS the author stated in an earlier publication, [1] he is confident that whatever conditions are ultimately proved to be manifestations of the saccharine disease, the primary Escherichia coli infections will certainly be amongst them. Such infections, in his opinion, play the dominant role in appendicitis and in primary infections of the urinary tract, and an important role in cholecystitis and diverticular disease. With the urinary infections he includes symptomless bacteriuria. In his opinion all these conditions stem from the presence of a quite abnormal number of these organisms in the intestines, due to an unnatural food surplus occurring there, which provides their sustenance. This food surplus arises partly from the eating of food that is not truly desired, as will be explained in Chapter X, but mainly from the consumption of refined carbohydrates. The author has already tried to show (in Chapter II) that the refining of carbohydrates leads to deception of the sensations of taste and satiety, and to over-consumption; and hence to the presence in the intestine of the food surplus just described, with its inevitable effect on the bacterial population.
Nor must sight be lost of another point. Raw foods are resistant to bacterial decomposition, inasmuch as the cells constituting such foods are, or recently were, alive. There is no need to discuss here the biological mechanisms involved in this resistance; what matters is that such resistance is not present in inert foods, like refined sugar. Thus the sugar present in portions of sticky sweets lodged between the teeth will be fermented much more quickly than that present in pieces of raw fruit lodged in the same position. And this reasoning has much application even in the intestine, as practical experience has taught; this will be touched on below.
Undoubtedly an excess of organisms other than the E. coli is generated by the above food surplus, but we take the E. coli as the type organism, some strains of which are known to grow particularly well in the presence of certain sugars such as glucose, and which is also known to possess pathogenic powers when present in excessive numbers. Such attack would be fostered by any abnormality present, necessarily lessening the perfect adaptation in the tissues, such as stasis in the appendix, undue acidity in the urine, or excessive cholesterol in the bile (all of which have been shown, or will be shown, to be related to the same refined diet).
That the intestinal flora vary greatly on different diets is well recognized. Thus Dubos and Schaedler [2] in a paper in 1962 on their work in this field at the Rockefeller Institute, New York, conclude with the following: ‘Walking in Metchnikoff’s footsteps, once more, we are inclined to believe that the usual intestinal flora is an expression of man’s total environment, and that its control may turn out to have as profound effects on the well-being of human infants and adults as it has on the growth of mice and of farm animals.’
In the author’s view the part of the total environment overwhelmingly involved in this matter is the diet, and, as regards the conditions now under discussion, some of these, such as appendicitis, may follow hard on dietetic excesses.
Mention of Metchnikoff in the above quotation leads again to the frequently offensive odour of the stools in civilized man and when the nose signals offensiveness it signals the presence of noxious materials, for else evolution would have resulted in a needless response. This odour is in sharp contrast with that of the stool in any wild creature, which, though often characteristic of a species, is never offensive. Chapter II noted that Eskimoes use the faeces of the reindeer as a vegetable. Another example is provided by the difference between the stools of breast-fed infants, which are acid in reaction, with the Bacillus bifidus predominant, and which smell like ‘bread in the oven’, and those of infants fed on artificial mixtures, often containing heavy loads of sucrose, as was shown in Chapter VII, which are alkaline in reaction, with the E. coli predominant and of which ‘the smell is putrefying’ [3, 4, 5]. All these differences in odour can logically be ascribed to the bacterial decomposition of the food surplus just mentioned, in the gut of civilized man, which surplus does not materialize under conditions of natural feeding. In this decomposition of an unnatural food surplus, by the E. coli and allied organisms, with the production of evil-smelling indole, skatole, and related products (from the breakdown of proteins, but accelerated by the presence of glucose in the medium ), is seen the basis of an intestinal toxaemia, such as was long ago formulated by Ehrlich, and pursued by Metchnikoff, and which is certainly not lessened by any stasis in the gut due to the same refined diet. The author therefore regards an unpleasant odour in the stools and in the flatus as an important index, on the one hand of potential bacterial invasion from the gut, and on the other of a possible toxaemia originating in the same site.
Those who would contest the power of refined sugar, when eaten, to cause a very rapid proliferation of certain intestinal micro-organisms, such as certain strains of E. coli, have to explain the undoubted fact that within, say, 4 hours of eating a mixture of sugar with protein, as happens, for example, in the taking of a jam omelette, highly offensive flatus begins to be passed and may continue for some hours. With a plain omelette, followed by some raw fruit, this sequel does not take place, assuming both are eaten in conformity with the appetite. The explanation of the difference lies partly in the surplus of sugar eaten in the first case, but also partly in the antibodies present in the raw fruit, as explained above, in the second case. The author himself attaches the utmost importance to this difference, in many treatments. It is also mentioned on the diet card at the end of this volume.
Meanwhile let us consider the reasons for believing that the primary E. coli infections are manifestations of the saccharine disease.
1. Racial Considerations
The first reason is based on the rarity of these infections in many primitive peoples, which is already well recognized. For example, we may quote the following statement on appendicitis from Boyd’s standard work on pathology. [6] ‘The disease is common in highly civilized countries and urban communities, but rare in remote rural districts and among primitive peoples. During the nine years that McCarrison practised among the hill tribes of the Himalayas he never saw a case of appendicitis. Natives who live on a diet abundant in cellulose are immune from the disease, but when they adopt the diet of civilization they lose that immunity.’
The author and G. D. Campbell collected some evidence on this subject, taking as material those Africans still living tribally, referred to in earlier chapters of this work. The figures in Table III were kindly supplied as representing the admissions for these complaints to the Charles Johnson Memorial Hospital, Nqutu, and the Eshowe Hospital, both mentioned previously as serving the tribal Zulu populations of Natal.
|
Table III
A Comparison of the Incidence of Appendicitis, Cholecystitis and Gall-stones, and Diverticulitis in Tribal Zulus and in N.H.S. Hospital Patients |
|||||
| Appendicitis | 23 | 0.18 | 24 | 0.09 | 3.2 |
| Cholecystitis and gall-stones | 3 | 0.02 | 5 | 0.02 | 0.7 |
| Diverticulitis | Nil | Nil | Nil | Nil | 0.3 |
It emerges from Table III that the incidence of even the commonest of these conditions in tribal Africans, appendicitis, is only 3-5 per cent of the incidence of the condition in English hospitals, and of the other conditions much less again.
As regards E. coli pyelonephritis in tribal Africans, this is very rare in the male (where such an apparent infection nearly always turns out to be secondary to bilharzia), but is not uncommon in the female. It is difficult to understand why an E. coli infection, so rare at other sites, as shown above, should not be equally rare at this one. The explanation that would at once be given in Natal is that these are ascending infections from below, and stem from lack of hygiene at the outlet of the female genital tract, especially in connexion with coitus. Though such facts in these Africans are undoubted, this explanation is not easy to tie up with evolutionary principles, but the subject cannot be pursued further here.
It will be recalled that these Africans are subsisting mainly on unrefined maize, with up to recently a striking absence of refined carbohydrates, though the picture as regards sugar is now rapidly changing, as indicated earlier.
In this respect it must be emphasized that the above figures by no means indicate that these E. coli conditions are found, even to the very limited extent shown, in those who eat unrefined carbohydrates. For the patients involved may well have been getting at just these foods, and the author has no doubt that careful questioning would reveal that this was exactly what they were doing. Thus, A. Barker, [8] Superintendent of the Nqutu Hospital, in a letter to The Lancet (1964): ‘Recently as a result of government policy, a group of 4000 Zulus have been moved into this district from where they had formerly lived, near one of our larger towns in Natal. Patterns of disease amongst these folk — who eat white bread, buns, and fish and chips, and drink aerated waters — differ notably from those to which we have become accustomed amongst rural Zulus… Perhaps this small group represents a control against which can be judged the benefits of the simpler diet of the still tribal Zulu?’
Turning now to Africans living in the towns in Natal, such as Durban, all the above diseases are commoner in them than in their tribal cousins, but it will be more illuminating to turn at once to the Negroes in the United States, who have had a longer and more complete exposure to the consumption of refined carbohydrates, and in whom, therefore, the differences in incidence should prove sharper. And with regard to this, a review of the literature leaves little doubt that any difference today in the incidence of these E. coli conditions (appendicitis, cholecystitis, and pyelitis) in the Negro and the white is unimportant. In short, there is every indication that the evidence from the Negroes in the United States is no less revealing in these E. coli conditions than it has already been shown to be in the conditions studied earlier in this work.
2. Historical Evidence
The second reason for believing that the primary E. coli infections are manifestations of the saccharine disease lies in the increase in the incidence of these conditions in Westernized countries like our own, over the last century or so, during the time of the great rise in sugar consumption. This increase in incidence is not nearly so easily established as in the case of, say, duodenal ulcer or dental caries, and indeed lacks full statistical proof. Nevertheless, such increase is widely held to have occurred, and the author is not the first to relate it to sugar consumption. Thus, as long ago as 1938 Brown [9] advanced this relationship in the case of appendicitis, contending that the main rise in the incidence occurred between 1880 and 1900, during which time the consumption of sugar in the United Kingdom rose from 60 lb. per head per year to about 90 lb. Similarly Cecil and Loeb’s Textbook of Medicine: [10] ‘Appendicitis was present but relatively rare in civilized countries until the end of the nineteenth century, but from that time till the middle thirties of this century a pronounced increase in cases has occurred.’
This increase is well seen in the following figure (Fig. 7) for admissions to the Radcliffe Infirmary, Oxford, kindly given to the author by Mr. A. Elliot-Smith, who also provided the following note: ‘Disease arising in the appendix was recognised during the nineteenth century and there are many published accounts, including post-mortem findings. In the middle years of the century many cases were wrongly ascribed to primary disease of the caecum; hence the term “typhlitis” or “perityphlitis”. However, if all such cases are collected together as possibly or probably due to appendicitis, the total incidence up to about 1890 is not high. Lister’s work on antisepsis and improvements in anaesthesia made surgery safer, and in particular acted as a great stimulus to the development of abdominal surgery, so by the end of the century more operations were being performed than previously. But taking all these factors into consideration, and the natural increase in population, there still appears to have been a very considerable and relatively sudden increase in the number of cases of the disease around the turn of the century.’
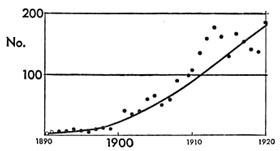 Fig. 7. — Number of cases of diagnosed appendicitis admitted to the Radcliffe Infirmary, Oxford, 1890-1920. (Total number of patients: 1900: 2200; 1910: 2370; 1920: 2260.) |
Since the recent death of his friend and collaborator, Mr. A. Elliot-Smith, the author has received the aid of another friend and collaborator, Dr. Walter Yellowlees, who has kindly supplied the chart reproduced below (Fig. 8) for the appendicitis operations in the Edinburgh Royal Infirmary around the turn of the century.
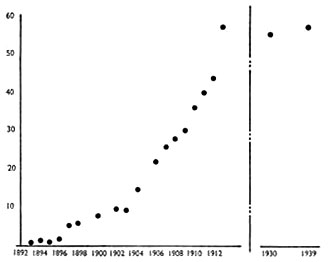 Fig. 8. — Operations for appendicitis, Edinburgh Royal Infirmary. Appendicectomies per 1000 total admissions, 1892-1913. (Source: ‘Edinburgh Hospital Reports — Archives Department — Royal Infirmary, Edinburgh.’) Figures for the years 1899, 1901, and 1905 are not available. |
It may be added that A. Rendle Short, [11, 12] as long ago as 1920, attributed the rise in the incidence of appendicitis towards the end of the last century to the consumption of white flour, but specifically excluded from the causation the consumption of sugar. As carefully set out in Chapter II, this attribution would make the emergence of the disease about 100 years out, and in the author’s opinion is the exact reverse of the correct relative attribution.
3. Results of Treatment
The author is confident that the basic treatment of all the primary E. coli infections, when not calling urgently for antibiotics or for urgent operation, lies in ‘starving out’ the abnormal number of these organisms in the gut, by attacking the food surplus sustaining them there. This can be accomplished by the diet set out at the end of the present work, which reduces the carbohydrates in the food to their natural, unconcentrated level — and it is carbohydrates that form an important pabulum of the E. coli.
It was by clinical experience that the author came to hold this to be the mechanism of production in E. coli infections. He found, during 3 years’ service in the Royal Naval Hospital, Hong Kong, 1936-9, that these infections, mainly of the urinary tract, were exceedingly common. This was especially the case during the hot season, and it became borne in on him that the cause probably lay in over-nutrition. This was only too liable to occur anyway at this season, because the need for calories was reduced not only by the heat but also by the lightened duties of the sailors at this time; meanwhile inquiries revealed surprisingly little reduction in their food consumption (which may perhaps best be explained by the force of habit). He was, however, already convinced of the danger of over-consumption with refined carbohydrates, and it was clear that this danger would certainly become greater in the above circumstances.
When, therefore, these patients were admitted to his wards, he adopted the procedure of reducing their food to the natural, unconcentrated level. This was achieved by a diet of mashed potatoes, boiled in their skins, with butter and salt to taste, plus any fresh fruit and vegetables available. This diet was by no means unpopular and the results were very favourable indeed. There were of course no antibiotics in those years, but it was unusual for the temperature not to fall to normal, and for the frequent haze in the urine not to clear, in a matter of days. The potato skins and the fibre in the fruit and vegetables helped any constipation, but the author found that any purgative caused an immediate flare in the temperature, which he is confident was due to the greater fluidity in the gut fostering bacterial activity. Where necessary, therefore, he dealt with any accumulation by means of an enema, which provoked but little reaction. Subsequently a diet card similar to the one at the end of this work took care of any trouble that way. It is noted on this card that the most delicate test of the correct following of the diet lies in the disappearance of offensiveness from the motions and flatus, and to this the author attaches great importance.
It is extremely difficult in these days of rapid resort to antibiotics to advocate this natural approach to these infections in many cases, but it is self-evident that the human body is not designed to need antibiotics to keep itself free from attack by the E. coli organism; and as regards any part played by hereditary defects, it is worth recalling that none of these is known to occur more frequently than five times per 1000 births. One must also recall the epidemiological evidence given above. Therefore the author is confident that the natural approach in treatment, aimed at cutting out over-nutrition, will yield a very big reward in primary E. coli infections, particularly those of the urinary tract, and constitutes a further piece of evidence for including these infections as saccharine manifestations.
However, a very personal effort by the physician is at first essential, involving a careful explanation to the patient and careful attention to his likes and dislikes over food. For a food surplus in the bowel can almost as easily arise from eating natural food that is not desired as from eating unnatural food that is desired. Both aspects of the diet are important, and the card just mentioned aims at securing both.
In connexion with this natural approach in the treatment of E. coli infections, the author is privileged to include here a personal communication from Mr. Conrad Latto, who has provided invaluable personal assistance to the author in the matter of these treatments (Royal Berkshire Hospital, 15 March, 1973):
‘I have so far only had a limited experience with the natural, unconcentrated diet in E. coli cases, having tried it out in about ten patients. They have all been doctors, doctors’ wives, or nurses — i.e., people who could thoroughly understand the principle involved, and were able properly to carry it out. All without exception have benefited, and the lives of two doctors’ wives, one doctor, and two nurses have been completely transformed by this simple régime. It will be understood that what is concerned is not so much a cure as a perpetual prevention. If the natural diet is departed from, the trouble will return. This pilot study serves at the moment only as a pointer for the future, but it is intended to develop it much farther.’
On the Causation of Gall-stones
In previous publications [13,14] (and in the previous joint work) the author has always accepted the view of earlier physicians and surgeons — that cholecystitis and gall-stones mainly arise from infections of the biliary tract with the E. coli organism (large solitary cholesterol stones, however, probably being of metabolic origin). The infective view was expressed by Lord Moynihan in his well-known aphorism that every gall-stone is a memorial to the bacteria entombed within it. The author therefore regarded gall-stones as a manifestation of the saccharine disease, being caused by the E. coli organism just as in appendicitis and primary infections of the urinary tract (themselves regarded by him as saccharine manifestations).
However, Dr. K. W. Heaton [15,16,17] has largely changed the author’s mind in this respect. He has marshalled compelling evidence that gall-stones arise from the liver secreting an excess of cholesterol in the bile and/or a deficiency of the accompanying bile-salts (which normally hold the cholesterol in solution). He has advanced that these changes in the bile arise from the consumption of the same refined carbohydrates incriminated by the author, but with him the over-consumption is responsible, not for supporting a swarm of intestinal organisms that otherwise could never be there, but for the liver secreting too much cholesterol into the bile; and the loss of fibre is responsible, not for intestinal stasis allowing extra bacterial proliferation, but for intestinal stasis allowing extra bacterial conversion of a major bile-salt (chenodeoxycholate) into lithocholate, a substance believed to be able, after absorption, to depress bile-salt synthesis by the liver, and hence the solubility of cholesterol.
The present author, with his devotion to simplicity, is as much attracted by the first alternative (over-production of cholesterol) as he is repelled by the second (under-production of bile-salts). But given his conversion to the former, he cannot help contending that there is frequently room here for a synergistic causation, which includes infection by the E. coli organism as well. When he considers other enclosed areas in the body, like the urinary tract, the appendix, and any diverticula of the colon, and their particular vulnerability to attack by these intestinal organisms when present in abnormal numbers, often disseminated as they are by the blood-stream, and especially when he considers the enormous prevalence of these infections in Westernized countries today, he is particularly led to believe in this synergistic causation of many, if not most, gall-stones, at least those of the ordinary multiple type. And all the more so since attack by the E. coli organism is always rendered more likely by the presence of any unnatural factor in the area concerned, lessening the perfect evolutionary adaptation present, whether such factor consists of unnatural acidity in the urine (as will be shown later), unnatural stasis in the appendix, or unnatural amounts of cholesterol in the bile.
With regard to the second view above, concerning gall-stones and intestinal stasis, the author considers that as well as not being simple, this view would lead to the idea that gall-stones were caused by loss of fibre directly, instead of indirectly via over-consumption, as set out in Chapter II. Not only would the former causation land gall-stones amongst the wrong group of associated diseases, as set out in that chapter, but also it would lead to the wrong treatment, as likewise set out there. For treatment by bran, instead of by a ruthless attack on sugar consumption through the substitution of natural fruit, etc., would fail just as surely in gall-stones as it would in the other conditions caused by over-consumption, such as obesity and diabetes. It is also worth recalling from Chapter II that gall-stones, together with obesity and diabetes, have recently shown a startling increase amongst Canadian Eskimoes, who not only for practical purposes never ate any fibre in the past and so cannot be short of it now, but also whose sugar consumption has recently risen to over 100 lb. per head per year.
Meanwhile, there is the strongest collateral evidence for including gall-stones in the saccharine disease. Thus, epidemiological evidence includes the rarity of this condition in populations still living on unrefined carbohydrates, as already shown in tribal Africans (see Table III, above), but the rapid appearance of the condition when such Africans replace these carbohydrates by refined ones, on taking to the towns. In close accord with this is the present approximating of the incidence of gall-stones in the cousins of these Africans, the Negroes in the United States, to that in the white inhabitants in that country. [18] It is also remarkable that in the outbreak of the saccharine disease now taking place, as described earlier (Chapter II), amongst the Canadian Eskimoes, consequent on their sugar consumption rising to over 100 lb. per head per year, as they forsake their nomadic way of life and take to the new townships, gall-stones have suddenly become so prominent that surgical operations for their removal now exceed in these people any other operation of importance. And similar, if less striking, evidence is available from amongst the professional classes in Japan; [19] and from amongst the American Indians [20] who, with a high consumption of sugar, now have the highest incidence of gall-stones of any community in the world.
As regards historical evidence, Dr. K. W. Heaton, [16] who subscribes to the author’s saccharine conception and has provided him with valuable support for it, not only over the biochemical formation of gall-stones, arising from the consumption of refined carbohydrates, set out above, but also over the historical evidence for this causation, now under scrutiny, has shown how postmortems reveal the steady increase of this condition over the past half-century in Westernized countries. He has also shown with C. Holland [21] that the number of operations for removal of the gall-bladder reveal this increase to be particularly striking since the Second World War, not only in England, Sweden, and the United States in general, but also around his own city, Bristol, in particular. He has also shown that, accompanying this more recent increase, there has been a steady fall in the age of onset of gallstones, so that in Sweden they are now not uncommon even amongst children. These studies find support from the Registrar-General’s Reports on the Hospital In-patients Enquiry, and the whole march of events recalls similar happenings in dental decay, obesity, and other more complex saccharine manifestations.
K. W. Heaton [17] in his published work has also shown that experimental evidence, with laboratory animals, strongly supports gall-stones as being a saccharine manifestation. Thus, ‘all diets which have been successful in producing gall-stones in such animals have contained a high proportion of refined sugar or refined starch’.
Finally, as regards the clinical associations [22] of gall-stones, such as obesity, diabetes, and coronary thrombosis, which the author holds to be so revealing, these have been set out already in Chapter II.
II. Other Conditions
In the author’s opinion the following conditions merit the closest attention, as probable manifestations of the saccharine disease.
Toxaemia of Pregnancy
This condition might well arise from the gut, on the Ehrlich model mentioned earlier, through the bacterial decomposition of a food surplus there, stemming from the eating of refined carbohydrates and aggravated by a coincident stasis from the same cause. The best example of the rarity of this condition in the past in peoples not eating these refined foods has been, in the author’s opinion, recorded by E. H. Hipsley, [23] to whose paper, and to whose personal communications, he is wholly indebted:
‘In 1950 Bell and Wills noted a pronounced racial difference in the incidence of eclampsia between the indigenous Fijians and the Indians living in Fiji. In the three years 1947-9 there were 18 cases of eclampsia in 1106 Indian confinements, while there were no cases in the same period in 717 confinements of Fijians. In 1949 there were 27 cases of pre-eclampsia in 416 Indian confinements, but no cases in 266 Fijian confinements.
‘The indigenous Fijians and the Indians living in the Fiji Islands are each a well-defined racial group differing widely in social, religious, and dietary habits. Such a situation seems to offer a unique opportunity for the study of the dietary background of the disease. The staple food of the Fijian is a starchy fruit vegetable of which relatively large quantities are eaten, together with banana, coconut, papaw, leafy greens, and small quantities of meat, fish and crabs. The important foodstuffs in the Indian diet are flour (sharps), white rice, coconut oil, ghee, sugar, with small quantities of dhal, meat, milk, vegetables, and fruit. The bulk of this diet consists of the refined foodstuffs, white rice and flour (sharps).
‘Meanwhile as regards Southern India, where refined carbohydrates in the form of highly polished rice form the staple diet, obstetricians are unanimous in stating that eclampsia is very common there, and much more common in the cities than in the rural areas. Dr. Sunanda Bai, an obstetrician who has worked in both the southern and the northern provinces of India, states (1952) that eclampsia is much less common in the northern provinces, especially in the Punjab, “where the diet is much better balanced and contains home-pounded wheat”.’
In addition to the above, Hipsley describes an attack of eclampsia, of almost epidemic proportions, accompanied by a high incidence of beri-beri, in Hong Kong during the last war, which immediately recalls the peptic ulcer outbreak there described in the previous work on that disease (and mentioned cursorily in Chapter X of this one).
Hipsley considers eclampsia in some way related to a low fibre-content in the diet. From the author’s point of view this places the condition right in the saccharine group, and his conviction is not lessened by the present attention to obesity as a possible aetiological factor, since this is just the type of associated condition that his conception would envisage.
Certain Skin Conditions
There appears to be no doubt that some skin conditions are also manifestations of the saccharine disease. The relationship of many cases of eczema, especially in children, to the consumption of sugar, sweets, and confectionery is well known, and in the author’s opinion chronic furunculosis is the surest sign of high sugar consumption and is most quickly arrested by stopping it. (Styes and recurrent axillary abscesses, however, seem much more related to lowered resistance from physical over-exhaustion.) These and certain other skin conditions may exemplify the general effects of the intestinal toxaemia discussed earlier in this chapter, just as pruritus ani may exemplify the local effects. [24]
As regards acne vulgaris, which the author also relates to sugar consumption, it may be added for interest that this condition has suddenly become conspicuous in the Canadian Eskimoes referred to in Chapter II. Dr. Otto Schaefer, in reporting this event, and the sugar consumption behind it, has said: ‘Many Eskimoes themselves blame their pimples on the “pop, chocolate, and candies” the youngsters consume, as if addicted. One wonders what these people and the other old Northerners would think if they were to read some recent medical publications, in which dermatologists belittle or deny the role of dietary factors in the pathogenesis of acne vulgaris.’
Renal Calculus (Upper Ureteric Calculus)
The consumption of refined carbohydrates, whether in the form of sugar, white flour, or polished rice, may play a decisive role in the formation of renal calculus, as pointed out by the author in 1956.[25] It is well known that the precipitation of urates and oxalates is largely dependent on the degree of acidity in the urine — and this acidity in its turn is largely dependent on the type of food eaten. The consumption of refined carbohydrates bears directly on this sequence, for such consumption can lead to a marked rise in the acidity of the urine. The simplest example of this rise is seen in the case of eating refined sugar instead of sugar occurring in its natural form, such as in raw fruit. For nearly every type of fruit has an alkalizing effect on the urine, and especially is this true of acid fruits, due to the dissipation of acid groups as carbon dioxide via the lungs and elimination of alkaline groups via the urine. When, therefore, sugar is taken as a refined product, this alkalizing effect is lost. (It should be added here that this unnatural acidity in the urine may play a big part in its invasion by the E. coli organism, as already referred to above.) It must be added to the foregoing that replacing sugar, sweets, etc., by natural fruits and sweet vegetables renders the urine, through the high water-content of these fruits and vegetables, noticeably more dilute, the bearing of which on calculus formation is obvious.
In this respect the author would like to refer to the great rarity of renal calculus in tribal Africans, subsisting on unrefined maize, like the tribal Zulus, which rarity is everywhere acknowledged. He would also like to refer to a paper by A. J. Wing and others, [26] as recently as 1971, showing that African women in Kampala pass a significantly more alkaline urine than European and Asian women there, which these writers attribute to the staple consumption of green plantain bananas by these Africans. They consider that this alkalinity accounts not only for the low incidence of urinary calculi, but also for the low incidence of E. coli infections in many Africans.
However, renal calculus is also rare in most urbanized Africans, and in the author’s opinion this is because their diet is still only semi-Westemized. For example, their sugar consumption is only about a third of ours. This diet has recently been comprehensively documented. [27] What happens when the diet is fully Westernized is best seen in the United States Negro. Thus, in a valued personal communication to the author in 1965, D. M. Kozoll, writing from the Cook County Hospital, Chicago, states: ‘Our experience at the Cook County Hospital would indicate not only that renal calculus occurs in the Negro as frequently as in the white race, but also that in the female there seems to be a preponderance…’
The author has no doubt that if the consumption of refined carbohydrates is the primary cause of renal calculus, other modifying factors may be present in the incidence, as he explained in the chapter on coronary thrombosis. For example, it is clear that excessive perspiration in hot countries will aggravate the tendency to precipitation in the acid urine, though Surgeon-Commander N. J. Blacklock, [28] in a paper in 1965 on urolithiasis in the Royal Navy, has shown that in about 50 per cent of cases developing calculus in hot countries, previous service in these countries had no such consequence, thus underlining the presence of a deeper cause in the aetiology. This same paper likewise draws attention to the presence of obesity in cases of renal calculus.
But what the author finds, himself, to be of perhaps the greatest interest of all in this disease is the observation, made by various urologists throughout Europe, that the incidence of renal calculus has shown a significant rise in their respective countries since the turn of the century. So much is this rise an established fact that it is referred to in the literature as the ‘stone wave’, e.g., [29].
The best-documented study known to the author of this rise is that by D. A. Andersen in his Survey of the Incidence of Urolithiasis in Norway from 1853 to 1960. [30] He is grateful for permission to reproduce here one of the most critical graphs (Fig. 9). It is highly relevant to the present author’s conception that D. A. Andersen in his paper, partly as the result of the fall in incidence during the war years, considered that a major dietetic factor may be involved in this rise, perhaps related to the rise in the standard of living over the years. Be this as it may, ‘stones of the upper urinary tract, which were probably generally rare a century ago in Norway, have altered in incidence from being in 1911 the least common of the six abdominal diseases studied to become nearly as common as appendicitis or peptic ulcer, and if present tendencies continue, they may become the commonest hospital surgical abdominal disease in Norway’.
 Fig. 9. — ‘Surgical incidence’ of stones in the upper urinary tract, Correction II, Ullevål Hospital. |
References
1. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 40, 116.
2. Dubos, R., and Schaedler, W. (1962), Amer. J. Med. Sci., 244, 265.
3. Naish, F. C. (1948), Breast Feeding, 95. London: Oxford University Press.
4. Ellis, R. W. (1960), Diarrhoeal Diseases of Infancy, 295. Edinburgh: Livingstone.
5. Snyder, M. L. (1940), J. Infect. Dis., 66, 2.
6. Boyd, W. (1947), Textbook of Pathology, 526. London: Kimpton.
7. Hospital In-patients Enquiry (Ministry of Health and General Register Office), 1961. London: H.M.S.O.
8. Barker, A. (1964), Lancet, 2, 970.
9. Brown, A. (1938), Brit. Med. J., 3, 635.
10. Cecil and Loeb, Textbook of Medicine (1959), 11th ed., 984. Philadelphia and London: W. B. Saunders.
11. Short, A. Rendle (1920), Brit. J. Surg., 8, 171.
12. — (1946), The Causation of Appendicitis. Bristol: Wright.
13. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 42, No. 2, 55.
14. — (1962), Peptic Ulcer. Bristol: Wright.
15. Heaton, K. W. (1972), Bile Salts in Health and Disease. London: Churchill Livingstone.
16. — (1973), Clinics in Gastroenterology, Vol. 2, No. 1, 67.
17. — (1973), ‘Gallstone Formation’, in 9th Advanced Medicine Symposium (ed. Walker, J. G.). London: Pitman Medical.
18. Cunningham, J. A., and Hardenbergh, F. E. (1956), Archives of International Medicine, 97, 68.
19. Nakayama, F., and Miyake, H. (1970), Amer. J. Surg., 120, 794.
20. Sampliner, R. E., Bennett, P. H., Comess, L. J., Rose, F. A., and Burch, T. A. (1970), New Eng. J. Med., 283, 1358.
21. Holland, C., and Heaton, K. W. (1972), Brit. Med. J., 3, 672.
22. Kaye, M. D., and Kern, F. (1971), Lancet, 1, 1228.
23. Hipsley, E. H. (1953), Brit. Med. J., 2, 420.
24. Tucker, C. C., and Hellwig, C. A. (1937), Arch. Surg., Chicago, 34, 929.
25. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 40, 116.
26. Wing, A. J., Gunstone, D., Njema, D., and Shani, H. G. P. (1971), Afr. J. Med. Sci., 2, 329.
27. Lubbe, A. M. (1971), S. A. Medical Journal (Supplement — S. A. J. of Nutrition, 20, Nov. 1971).
28. Blacklock, N. J. (1965). J. Nav. Med. Serv., 51, 99.
29. Sallinen, P. (1959), Acta Chir. Scand., 118, 479.
30. Andersen, D. A. (1966), J. Oslo Cy Hosps, 16, 101.
Chapter X
Peptic Ulcer
PEPTIC ulcer is another condition that is considered here to be an unequivocal manifestation of the saccharine disease, and one that lends itself particularly well to the approach set out in Chapter I — embracing the law of adaptation, and also the distinction between on the one hand bodily defect and on the other hand personal build reacting with a new environmental factor. This subject is dealt with very fully in a separate work, [1] but the main elements of the argument will be set out in this one (only the main references being given). Furthermore, certain rare forms of peptic ulcer such as occur after burns will not be included here, though they could easily be accommodated by the present conception.
I. The Prevailing Views on the Causation of Peptic Ulcer, Held Here to be Untenable
At the present time a widely held opinion on the aetiology of peptic ulcer incriminates the gastric (hydrochloric) acid as the primary cause. Now, though the virtual confinement of peptic ulcer to the stomach and duodenum, which are the only parts of the intestinal canal normally exposed to this acid, points to the acid as undoubtedly the agent involved in the production of ulcer, the law of adaptation excludes the acid altogether as a primary cause.
For this law indicates that the production of hydrochloric acid must be just as perfectly attuned to the requirements of the individual as is, for example, the power in his arms or his legs or any other part of his anatomy. Far from constituting a liability, the production of large amounts of acid in the stomach, passing under the term ‘hyperchlorhydria’, should be regarded as a most necessary asset. A powerful machine is useless unless it receives the right amount of fuel to run it. A powerful man is equally reduced to impotence unless his stomach produces the right quantity of acid to secure the digestion of the large amounts of food his energies require.
Yet, as stated above, opinion today is only too likely to exalt the hydrochloric acid to the status of a primary cause. Thus Illingworth: [2] ‘The inescapable equation of ulcer aetiology — acid-pepsin aggression versus mucosal defence — allows for certain differences in the pathogenesis of duodenal and gastric ulcer. In duodenal-ulcer patients, gastric secretion is characteristically higher, the acid-bearing (fundic) area of the stomach larger, the gastric mucosa thicker, and the parietal-cell mass greater than is usual in normal people (Cox, 1952; Card and Marks, 1959). Gastric-ulcer patients, on the other hand, often have normal or subnormal secretion and atrophic mucosal changes. It is thus understandable that an increase in acid and pepsin should be incriminated as the dominant aetiological factor in duodenal ulcer, and impaired mucosal resistance as the underlying cause of gastric ulcer.’
The only chance of a statement like this not being in open conflict with the law of adaptation lies in the possibility of an excess of acid (hyperchlorhydria), or a deficiency of mucin, being a hereditary defect. And what does that chance amount to? In .the opening chapter we saw that no hereditary defect occurs more often than 5 times in 1000 births. Yet peptic ulcer is now so common in this country that about 10 per cent of men and 4 per cent of women develop clinical evidence of the disease at some time during their lives, the post-mortem evidence being nearer 20 per cent for each sex. [3] In short, the incidence of peptic ulcer is over 20 times as great as that of any known hereditary defect.
Also, the view that the hydrochloric acid is the primary cause of peptic ulceration is quite incompatible with the historical and racial incidence of the disease, for peptic ulcer was rare before the turn of the century, [1] and is absent in certain communities even today, as will be shown later.
Another opinion on the aetiology of peptic ulcer incriminates the ‘stress’ of living under modern conditions. But this cause is just as incompatible with the law of adaptation as was the preceding one. For what does evolution involve but a struggle for existence that has continued from the dawn of creation, and is still continuing? Such struggle for existence, with its ceaseless killing of one individual by another, represents the quintessence of stress.
Furthermore this cause, also, will be seen to be quite incompatible with the historical and racial incidence of the disease.
However, although stress here is absolutely excluded as a primary cause of peptic ulceration, it will be shown later that it plays a part as an aggravating factor. This aggravating factor consists of disregard of the instinct of appetite, in eating food that is not desired. In this connexion stress will be seen to be important — but it can at once be nullified by attending to the instinct.
To sum up, as regards the causation of peptic ulcer, it is again considered that the body is not built wrongly, but is being used wrongly. And again the question is: in what manner is it being used wrongly?
II. The View Advanced Here on the Causation of Peptic Ulcer
Protein-stripping
In searching for a new environmental factor as the essential cause of peptic ulcer, it is necessary to refer again to ‘the inescapable equation of ulcer aetiology — acid-pepsin aggression versus mucosal defence’, quoted earlier in this chapter. This equation has so dominated medical thought that a third factor has been lost sight of — the natural defence against the hydrochloric acid provided by the buffering effect of the food. This third factor is of the greatest importance because, if the natural buffering by the food is reduced, and still more if it is removed altogether, it is clear that the mucous membranes are exposed to a much more serious attack from the acid than they are designed to support, and the whole of the above equation is upset. In this connexion it should be added that it is now known (as set out in the separate work) that the highest acidities in the stomach occur during digestion and not in the empty, resting state. Furthermore, the thin, distended wall of the stomach during digestion must operate against the mucosal defence, whereas the thick, non-distended wall in the resting state must operate in favour of that defence.
It is not difficult to see how, under modern food processing, this reduction in buffering power very easily occurs. For the only component of food that buffers the acid is the protein. Fats, starches, and sugars do not affect the acid at all. And in the refining of carbohydrates the protein is either seriously reduced or removed altogether. A little later it will be shown, in fact, that there is a remarkable correlation throughout the world between the consumption of these ‘protein-stripped’ carbohydrates and the incidence of peptic ulcer. Meanwhile, the extent to which the protein component is reduced, or altogether eliminated, in the refining of carbohydrates is shown in Table IV. [4]
|
Carbohydrate Foods
|
||||
| English wheat, wholemeal flour (100 per cent extraction) | 11.2 | 11.0 | 9.3 | |
| Rice (husked only) | 30.0 (average) | 10.6 | 7.3 | |
| Potatoes | Variable, about 4-16 per cent depending on the degree of slicing | 10.5 | Variable; suggested figure 9.5 | |
| Manioc tubers | 60.0 | 3.0 | 0.4 (tapioca) | |
| Sugar-beet | 100.0 | 12.0 (average) | 0.0 | |
It will be noted in Table IV that the protein removed is estimated in protein calories as a percentage of all the calories present. This method of estimation is essential, but the reason will not be discussed here; it is dealt with in the main work.
Protein-displacement
It has already been shown in Chapter II how the concentration produced in carbohydrates during refinement leads to deception of the tongue and of the appetite — and so produces over-consumption. This extra consumption tends to displace the consumption of other foods, which contain natural amounts of protein. In short, the refining of carbohydrate foods not only reduces the protein outright, but also leads to a marked increase in the consumption of these foods, so that to protein-stripping becomes added protein-displacement. Fig. 1 in Chapter II deserves re-scrutiny in this connexion.
Consequences of Protein-stripping and Protein-displacement
In Westernized countries like ours, where the total protein-consumption is high, neither of the above protein losses would probably have a serious effect on the neutralization of the gastric acid were it not for two other factors of great importance:
- The stripped foods are often consumed by themselves.
- The various parts of a meal largely remain distinct in the stomach.
1. As regards the first fact, consider any young couple in a cinema. In the middle of the performance they are only too likely to consume some sweetmeat, which will probably consist of almost pure sugar, with practically no protein at all. The calorific value of this sweetmeat is high and will result in a considerable secretion of gastric juice. The consequences will be that the membranes of the stomach and duodenum are exposed to almost completely unbuffered acid, often for several hours.
(Since these words were written, about 10 years ago, it is well known that there has been some fall in the incidence of peptic ulcer in this country, and that this fall has been chiefly in acute perforations. It is the author’s deep conviction that such fall has been due to the large replacement of cinema attendances during this period by television-viewing in the home, where the consumption of concentrated sweetmeats is likely to be replaced by that of ordinary balanced meals. In this connexion it is of great importance that in this country during the last war, when exactly the same consumption of packaged sweetmeats took place in the shelters during air raids, a dramatic rise in acute perforations was recorded in almost all the cities involved; and this rise disappeared when sweet-rationing was introduced later. Those who find these facts hard to believe should consult the author’s main work on Peptic Ulcer, where they are fully documented.)
Very similar events take place on other occasions, too, such as during ‘elevenses’, where some three hours after breakfast the almost empty stomach receives a cup of tea or coffee, often heavily sweetened with sugar but with very little milk, and therefore containing hardly any protein. Another example is provided by drinks of alcohol taken some time before meals, especially at cocktail parties. In all these cases the stomach is liable to be subjected to almost completely unbuffered acid, often for a long time. In civilized countries, therefore, there lies concealed, under the cloak of a respectable total protein protection, a protein protection that at certain times of the day is seriously deficient.
2. As regards the second fact, it cannot be argued that, where the protein calories have been heavily reduced in parts of a meal, though the total protein calories of the meal remain high, the same danger is not present. It may be very much present. Consider a meal where a glass of sherry (containing no protein calories) precedes a beefsteak, and a tinned fruit salad (containing only 1.5 per cent of protein calories) follows the steak. It cannot be argued that the gastric acid will be adequately neutralized in this meal, for the following considerations show that it will not.
In the first place, in any radiographic meal it is easy to see that every peristaltic wave carries some part of the meal straight into the duodenum. The first waves often fill the duodenal cap. It is not a fact that the stomach contents are churned up till an even mixture results, and then the pyloric valve is released and the whole meal projected onwards. In the second place, it has long been known to physiologists that the succeeding portions of a meal are arranged in corresponding layers in the stomach. [5] Nor does drinking affect these layers of food in the stomach, since fluids by-pass the food and leave the stomach almost immediately. Veterinary surgeons have discovered that all the above applies to animals, too. Fig. 10 shows this layering in the human stomach.
 Fig. 10. — Tracing from radiographs taken at the times stated after a normal subject had eaten 200 g. of fried meat ball without contrast medium, 50 g. mixed with neobar, and then 100 g. without. Tracing from Neilsen and Christiansen (1932). (Reproduced by kind permission.) |
To sum up: there is obviously a fundamental difference in the protection afforded to the gastric membranes, by say, 12 oz. of protein food divided equally between three meals and the same 12 oz. divided between two meals with almost none in the third meal, as often happens in civilized countries today; and, if this fact is admitted, it is possible to extend it, through the known occurrence of layering, just described, to cover parts of meals. It may be added that the loss of buffering power produced by the removal of the protein element in carbohydrates can be, and has been, measured. [6]
The refining of carbohydrates has other serious repercussions on stomachic digestion. Thus, the removal of fibre lessens the mastication necessary in the food, and hence lessens, too, its impregnation with the alkaline, buffering saliva. This greater or lesser impregnation with saliva makes it impossible to go simply by the protein calories in foods, as is shown in the main work on Peptic Ulcer. Thus an apple with 3 per cent of protein calories may be much safer than chocolate with 4 per cent of protein calories. Furthermore, the absence of fibre alters the gastric emptying time, making it slower in the case of white bread [7] but much quicker in the case of sugary solutions. Such factors make it extremely unwise to regard any deviations from the natural process as not serious, especially since such deviations may be endlessly repeated. If Life has taught the author anything, it is the danger of trying to be clever at Nature’s expense, as noted before in this work (see also Appendix).
Finally, it is not necessary to stipulate that the removal of protein leads to higher eventual levels of acidity in the stomach, for certain foods (including perhaps unrefined carbohydrates) may require for their digestion higher levels of acidity than others require (including perhaps refined carbohydrates). But what the removal of proteins certainly will do is to lead to these levels being reached in a quicker and more brutal manner which, though the mechanism involved is quite different, can impose strains on the defensive secretions of the stomach directly analogous to those produced by unnaturally concentrated carbohydrates on the insulin of the pancreas, as described in Chapter VII on diabetes. Furthermore, it is profoundly important, concerning this unnaturally rapid attainment of maximal acidities, that, as shown above, the stomachic contents enter the duodenum regularly all along the post-meal period, so that any insufficiently buffered acid strikes the duodenum right from the start.
III. Experimental Evidence
Supporting evidence for the foregoing has been published in a paper by J. E. Lennard-Jones, J. Fletcher, and D. G. Shaw [8] They showed in a series of test-meal studies that the climb in gastric acidity following the eating of refined-grain products is indeed considerably accelerated compared with that following the eating of their unrefined analogues. Their figure for this difference in the case of refined maize cornflour, as compared with whole-maize meal, is reproduced here (Fig. 11). This has a particular bearing as regards Africa, where so much maize is eaten. It is far the clearest of the present figures.
 Fig. 11. — Mean acidity of the gastric contents in 6 patients with duodenal ulcer after meals of whole maize and maize cornflour. (Reproduced by kind permission.) |
 Fig. 12. — Further studies in the buffering qualities of refined and unrefined carbohydrates. (By kind permission of Mr. F. L Tovey.) |
Fig. 12 shows similar differences in early buffering in the case of rice with, and without, the addition of bran, for which the author is grateful to his friend, Mr. F. I. Tovey, whose buffering studies have been invaluable to him. [6] It will be noted that unlike the studies by J. E. Lennard-Jones and others, just quoted, these latter studies showed higher eventual levels of acidity in the presence of bran. This particular difference in results, however, does not affect the author’s argument, which is not concerned with eventual heights of acidity, but with natural and unnatural speeds in the attainment of these heights. But there is a far deeper reason for this unconcern, which is that it follows, as an evolutionary axiom, that if a natural food, eaten with desire, generates a higher level of acidity, not only will this be harmless, but it should actually help the digestion of the natural food involved.
The author would like at this stage to present a small chart produced for him through the great kindness of Dr. John Temperley, now Consultant at the Preston Royal Infirmary, when he was working at University College Hospital some years ago (Fig. 13).
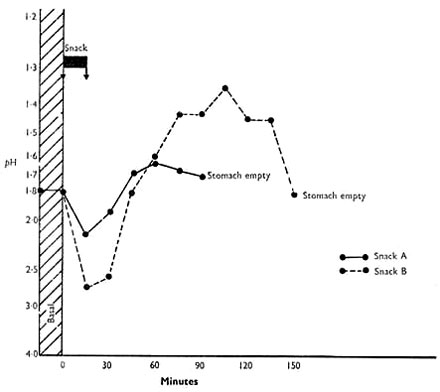 Fig. 13. — Similar studies in a solution of sugars compared with raw apples. (By kind permission of Dr. John Temperley.) |
Snack A: ‘Hy-cal’ (Beechams), 36.2 g., in water (67.5 cal., 126.7 g. H2O.
Snack B: 150 g. dessert apples, cored and quartered (67.5 cal., 126.7 g. H2O).
Graphs show pH of gastric contents after each meal. Mean of results in 4 patients with peptic ulceration.
It contrasts the average of the acid response in four subjects given a sugary (Beecham’s Hy-cal) solution with the response when they were given an equi-caloric quantity of cut-up raw apple. It will be noted that the two curves are utterly different. At first sight it would appear that the natural carbohydrate inflicts greater acid strain on the stomach than the refined carbohydrate, though it has already been pointed out that for evolutionary reasons any height of acid following a natural food, eaten with desire, cannot be harmful. In this case, however, two things are to be noted: (a) the initial buffering referred to earlier is far greater in the case of the apple, and (b) the emptying time of the stomach with the sugary solution is little short of half that with the apple. Indeed Dr. Temperley told the author that the passage of such sugary solutions through the stomach is so rapid that it is often difficult to get out the gastric juice through the Ryle’s tube to analyse the result.
Now the gastric acid is secreted at the fundic end of the stomach and is neutralized at the pyloric end and in the first part of the duodenum, where it meets the alkaline juices diffusing up from the second part of the duodenum. Therefore, with the above sugary solution there is not only much less time for the neutralizing mechanism to appear, but also much less time for it to act when it does appear. The completely different impregnation with saliva in the cases of the sugar solution and the apple is no doubt of great importance, too.
However, the author is convinced that the interference with the initial buffering is the main cause of the acid strain with the sugary solution. For according to McCance, [7] in the case of refined, white bread, the passage through the stomach is slower, not faster, than in the case of unrefined, wholemeal bread. The very rapid passage of sugar is presumably related to its ready solubility.
Meanwhile, the dangerous implications of sugar and sweets over the causation of peptic ulcer are obvious.
The author cannot agree with Mr. Tovey that a loss of some protective factor is involved in the causation of peptic ulcer by refined carbohydrates. The author believes that the causation normally lies directly in interference with the natural buffering of the hydrochloric acid, as set out above, and for the following reasons.
Firstly, the experience of the prisoners-of-war in Japan and elsewhere, many of whom are alive today, showed, as will be set out shortly, that the one thing the prisoners did not lack was fresh cabbage and other green vegetables, rich in such protective factors, which they grew for themselves. And yet the ulcer relationship to white rice was dramatic.
Secondly, assuming that careful attention is paid to the all-important dating of the observations (because of the stealthy spread almost everywhere of sugar, white flour, and white rice), the ulcer incidence all over the world can easily be related to interference with this buffering of the acidity through refining the carbohydrates. Especially is this true of the exceptionally high incidence of peptic ulcer where manioc (cassava) is eaten, where the incidence closely follows the varying interference with the protein buffer, dependent upon different modes of preparing different types of manioc, as will be described shortly.
Thirdly, peptic ulceration is confined to the stomach and duodenum, where hydrochloric acid is alone to be found. So it is simpler to deal with the acid and its neutralization than it is to introduce other factors. And the author is a strong believer in the empirical tendency of simple explanations to be correct explanations, as set out in the Preface.
Fourthly, Mr. Tovey attaches importance to the higher levels of acidity reached with certain natural foods — which levels the author, for the evolutionary reasons carefully set out above, cannot regard as ever being harmful.
* * *
We now pass to the geographical incidence of peptic ulcer, and to the evidence from the prisoner-of-war camps in Japan and Russia, to show the relationship of the disease to the consumption of refined, protein-stripped carbohydrates.
IV. Geographical Incidence of Peptic Ulcer
This is too big a subject for the author to do more than touch on here, but a few of the more striking examples will be given. Details are set out in the separate work. However, he regards it as most important, in reading the following paragraphs, to remember that peptic ulcers occurring in undeveloped areas of the world, though not subjected perhaps to as complete a diagnostic investigation as in more developed countries, still cannot remain hidden indefinitely. They are certain to reveal their presence in the end, either by perforation, or by haemorrhage, or by scarring and obstruction. Therefore the evidence put forward by responsible medical officers in these areas should be given every consideration.
Two further points must be added. The first is that medical observations in the past are likely to be rendered more, not less, valuable by any difference in comparable observations today. This is largely because of the rapid and stealthy spread of refined carbohydrates in so many parts of the world. Indeed, Westernization throughout Africa is taking place so fast that the Hans Snyckers Institute has been set up at the University of Pretoria, Republic of South Africa, to record before it is too late the previous absence in Africa — as established by earlier medical observers (including those still alive today) — of certain disease conditions now increasingly appearing there. Such an institute is of great importance, for otherwise these earlier observations are only too likely to be written off as erroneous, whereas it is nearly always these observations that are the most revealing.
The second point is an evolutionary one. It may be advanced as axiomatic, from evolutionary considerations, that any foodstuff in its natural, unaltered state — such as an unrefined grain, like the millet known as cholam, mentioned below — which occurs in a person’s natural environment and is eaten by him with relish, will not cause disease (including peptic ulceration). Therefore if, for example, eaters of natural cholam are getting peptic ulcer, then a personal glance at the larders in such sufferers’ homes might be needed to exclude the presence of sugar, white rice, white flour, and even manioc (tapioca), to say nothing of fermented liquors. Such a glance might well explain why peptic ulcer has been observed in the eaters of cholam in India, whereas it has been conspicuously absent in the eaters of the parallel guinea-corn in Nigeria (see below ).
Africa
In Africa the incidence of peptic ulcer follows very closely the consumption of refined carbohydrates. Thus in the Charles Johnson Memorial Hospital, Nqutu, A. Barker reports 2 cases of peptic ulcer in 25,000 in-patients over 10 years (1950-60). These Africans subsist almost entirely on unrefined maize, as described in Chapter VII.
Similarly, in the heart of Ethiopia, where the natives live on unrefined teff (a form of millet), the government radiologist, M. Tausjo, reports that only 2 out of 1000 patients suffer from peptic ulcer, and that these are almost invariably those who have been eating Westernized foods. But the situation there may be very different today, and even in 1960 peptic ulcer was common in Addis Ababa and other large towns in Ethiopia, where white flour and sugar were being consumed in ever-increasing quantities. This evidence, and much other evidence of the rarity of peptic ulcer in the eaters of unrefined grains, is set out in detail in the main work on Peptic Ulcer. For example, in northern Nigeria where the main food is practically always the unrefined millet called guinea-corn (the equivalent of cholam in India), E. T. Mess (1960) reports 2 cases of peptic ulcer (both causing pyloric stenosis) in the Wusasa Hospital in 12 years.
Per contra, the disease is just as common in the Negroes in the U.S. Army as it is in the whites, [9] though formerly it was rare in U.S. Negroes when they ate hominy, made from unrefined maize. In many parts of civilized Africa the disease is very common, too. Thus, the disease occurs frequently, in typical form, in Kampala and Nairobi, where refined carbohydrates are commonly eaten by Africans. The disease is common in southern Nigeria, too, where the diet includes large amounts of manioc, which, as shown in Table IV, has lost a large amount of its original protein.
In Durban the incidence of peptic ulceration in the Zulus is still a long way behind that in the white residents (which may be explained by the diet being only semi-Westernized). In the Natal Indians, with their higher consumption of sugar, the incidence has already risen to equal that in the white residents.
India
In India peptic ulcer occurs only in certain regions, being absent in others. This ulcer belt is well known. Table V shows how closely the incidence of ulcer follows the consumption of refined carbohydrates. [10, 11] (It is to be noted that the milling of rice leads to a loss of about one-third of the protein, whereas hand-pounding the rice cuts out much of this loss.)
|
Table V
The Relationship Between the Incidence of Peptic Ulcer and the Consumption of Refined Rice |
||||
| State | ||||
| Bengal | 51,087,338 | 16,976 | 33 | 25 |
| Madras | 46,740,028 | 57,397 | 1143 | 70 |
| Bihar | 23,676,028 | 8,851 | 37 | 10 |
| Orissa | 18,653,555 | 4,132 | 29 | 20 |
| Punjab | 23,580,852 | 2,131 | 9 | * |
| Assam | 9,247,857 | 926 | 10 | 15 |
| United Province | 49,614,833 | 4,460 | 11 | 15 |
| * Rice mostly replaced by unrefined wheat and maize. | ||||
The fact that this table might be superseded today is not important. The rapid and stealthy spread of sugar, white rice, and even white flour might well make nonsense of it. What is important is that the table existed once and that it points to the evolutionary axiom given above: that natural grain, like any other natural food taken from a man’s native environment, and eaten with desire, will not cause peptic ulcer; whereas refining the grain, or otherwise interfering with it, might well make it causative. Indeed, as stated earlier, before the author accepted any unrefined grain as a cause of peptic ulcer, he would want a search made of the sufferers’ abodes to eliminate the presence of sugar, refined rice or flour, alcoholic beverages, or even bitter manioc. Too often he has found that local statements are very unreliable in this respect, especially perhaps amongst Indians, where such statements may have other objectives in view, and the great essay by Macaulay on Warren Hastings confirms his feelings about this. Too often there is given the inquirer an answer that he wants to hear. A native can have extraordinary prescience in this respect.
Peptic ulcer is commonest of all, however, in the southwestern parts of India, such as Kerala, where manioc is consumed in large amounts. As already stated, Table IV shows that this carbohydrate has undergone serious protein-stripping, and the subject will be further considered below.
It may be added that no relationship whatever exists between the incidence of peptic ulcer and the consumption of hot curries, [12] or between the incidence of the disease and any form of avitaminosis. [13]
Indonesia, Malaya, and China
In 1930 Kouwenaar showed by post-mortem examination that 151 ulcers and scars occurred in 1370 Chinese immigrants in Sumatra against only 8 in 1300 Javanese men. [14] It can be shown that these Chinese were eating milled rice, bought in the bazaars, whereas the Javanese were eating hand-pounded rice in their own homes. Yet peptic ulcer at this period of time was reported very rare indeed in the Chinese living in China itself, whenever they were eating home-pounded rice. [1]
Japan
In Japan the consumption of refined carbohydrates, in the form of milled rice and also considerable quantities of sugar, reaches a very high figure — and the incidence of peptic ulcer is the highest in the world (34.7 per 100,000 as against 14.1 in England and Wales). [1]
V. A Note on Manioc Ulcer
Manioc (Cassava)
As the author has set down in his work on Peptic Ulcer, this potato-like plant is a native of South America, but in recent times has been introduced into other countries, such as India and Africa. It must also be stated that the tubers of most varieties of manioc (cassava) produce the highly poisonous prussic acid in their outer coat, as a protection against marauding insects. Therefore, before mankind can eat these tubers, he has to peel them, soak them (often after slicing) for a long time in water, and then throw the water away. This gets rid of the prussic acid, but the leaching also reduces the original 3 per cent of the protein calories to about 1.5 per cent. However, in the factories which process manioc to tapioca, the protein calories are reduced much more — to 0.5 per cent, indeed, or even less. Since the natives eating manioc are amongst the poorest of the poor and often eat relatively little else, it is not surprising on the view advanced in this work, relating peptic ulcer to the removal of protein from natural foods, that this disease often becomes rampant amongst them. This is notoriously the case in Kerala in India, where manioc was introduced in the latter part of the nineteenth century, and where a very high incidence of the disease obtains. The Belgians likewise introduced manioc into Africa, first before 1920 and more extensively after 1940, and P. Konstam [12,13] has shown how closely, as regards manioc production and ulcer incidence, southern Nigeria in Africa resembles Kerala in India.
There is also a very high incidence of peptic ulcer in Burundi in Africa, where manioc is likewise widely cultivated, and where local opinion has related the high incidence to the big introduction of the plant there in the 1940s. This dating, however, could obviously apply to other possible causes too, but it does appear to the author as significant that the type of ulcer met is of the chronic sclerosing duodenal type, as occurs with manioc consumption, and not of the ordinary Western type, sometimes causing perforation. Another type of refined carbohydrate is commonly consumed in Burundi, too, and that is home-brewed alcoholic beverages, but the author cannot, himself, forsake the idea of a substantial manioc causation of ulcer there, as would be expected in a country that, with Rwanda, produced, at least in 1956, some 2 million tons of this dangerous foodstuff, which under natural conditions the tongue would not allow to be eaten at all. He is indebted for much information about peptic ulcer in Burundi to Mr. George Hamber, surgeon at the Hôpital de Buye, Ngozi, but he must stress that the opinions given here are his own responsibility.
* * *
Meanwhile, a further vital point may throw more light on this subject, for to the south, in Kalene, in Zambia, though manioc is to a great extent the staple diet, hardly any ulcer is seen at all. Before offering his own explanation of this remarkable fact the author must first express his deepest gratitude to Dr. D. Fitzgerald Moore, formerly Senior Medical Officer of the West African Medical Service, for certain key information on the subject of manioc; and to Dr. Evelyn Nightingale, recently of the Kalene Mission Hospital, Zambia, and to her assistant there, Miss Hilda Wadsworth, S.R.N., for details of the preparation of manioc carried out in Kalene.
Briefly, it may be stated that as well as the bitter, poisonous manioc, there is also a sweeter manioc that is only slightly poisonous or not poisonous at all. Whilst much leaching is needed for the bitter sort, little or no leaching is needed for the sweeter sort. Now in Burundi most manioc is of the bitter sort and the tubers are first peeled, sometimes cut up, and then soaked for several days in water. But in Kalene most manioc is of the sweeter sort, and here the tubers are soaked in water for several days before they are peeled. Both maniocs are then dried, pounded, and the flour added to boiling water to make a mush or porridge, all of which is eaten.
In this sequence one is powerfully reminded of S. T. Thomas’s experience in India, set out on page 46 of the author’s work on Peptic Ulcer, where in Orissa almost no cases of peptic ulcer come from the hills, where the water that the rice has been boiled in is drunk, whereas a great many cases of ulcer come from the plains, where the water is thrown away. And this water is rich in leached-out protein.
It may be added to the above that a careful analysis of the manioc mush or porridge at Kalene, by the Senior Public Analyst in Sussex, has shown that it contains 2 per cent of protein, and even more on a calorie basis, which is considerably above the percentages mentioned above for bitter manioc after treatment.
VI. Evidence from Prisoner-of-War Camps in the Far East, 1942-5
Interesting evidence on the aetiology of peptic ulcer is provided by data from the Japanese prisoner-of-war camps which, as far as the writer knows, has not been used in this connexion before. In these camps the commonest element in the diet was rice, and usually highly milled rice at that. When little other food was provided the diet approximated, therefore, to that already described for certain parts of India and Indonesia, and if the present argument is correct, peptic ulcer should have become conspicuous. Per contra, if the rice or other grain was not highly milled — and sometimes it was not — then the diet approximated to one of unrefined cereal, with very little animal protein, as already described for certain parts of Africa and Asia, and peptic ulcer should have become rare, no matter how reduced in amount the rest of the diet or how unfortunate the general conditions. The facts are as follows:
1. Singapore and Thailand (Siam)
Here the rice issued was highly milled but was supplemented by an issue of rice polishings until the end of 1943, when the issue ceased. In 1944 duodenal ulcer, which up to then had been infrequent, became, in the words of Julian Taylor’s contribution to the History of the Second World War, ‘a plague’. [1]
Meanwhile, it is a remarkable fact that among the prisoners of war taken away from Singapore in 1943 to work in Thailand on the tragic Burma Railway project, where the captives lost over 40 per cent of their numbers before returning to Singapore in 1944, peptic ulcer was almost never seen, and it is of the greatest interest that the rice issued to these prisoners was either unmilled, or supplemented with rice bran (normally used in Siam for feeding the pigs).
2. Hong Kong and Japan
In Hong Kong the prisoners were fed on milled rice and peptic ulcer symptoms and perforations were prominent. However, after two years a large proportion of the prisoners were transferred to Japan itself and here an important change occurred in the diet, the prisoners being given either a mixture of unmilled grains (including barley and millet), called the ‘Korean mixture’, or red (unmilled) rice. On this diet peptic ulcer symptoms and perforations, for practical purposes, vanished, no case being seen in Tokyo in some 6000 prisoners for over one year, and only I case being seen in Kobe and Osaka amongst 7000-8000 prisoners during the same period. [15] Meanwhile among the native Japanese population, which was largely fed on highly milled rice, the incidence of the disease quietly doubled.
Of one thing the medical officers were very confident: the dramatic improvement in ulcer symptoms and perforations in Japan, on the ‘Korean mixture’, was certainly not due to the appearance in the food of the C vitamin or other protective factor of this type. For in the Hong Kong camps there was never any lack of green vegetables, such as cabbage, which the medical officers, like the other prisoners, themselves helped to grow (largely assisted by the rather primitive drainage system present in these camps), whilst in Japan such green vegetables, though adequate, were, as the author’s main work on Peptic Ulcer sets out, considerably reduced.
It may be added that during the above period Tokyo was almost completely destroyed by the U.S. B29’s, and extensive damage was done to Kobe and Osaka. In the raids on London and other English cities a big rise in perforated ulcers occurred, [1, 16] as already described, which is in striking contrast to what happened in the Japanese camps. Quite clearly this difference cannot be explained by any form of stress argument.
The above key evidence from the Japanese prisoner-of-war camps was carefully recorded [15] by the author’s brother, Surgeon-Captain H. L. Cleave, F.R.C.S., who was himself a prisoner and was in surgical charge of most of the prisoners, both in Hong Kong and Tokyo, and to whom the author is indebted for this and much other help in the preparation of the present volume.
3. Dutch East Indies
The Japanese prison camps in this area were investigated by a Dutch medical team in 1945-6, sent out by the Netherlands Red Cross, a full report of whose findings is published. In this report the rarity of peptic ulceration is noted — these prisoners were nearly all fed on red, unmilled rice. [17]
It will be noticed that in spite of other variables in these camps, which tend to cancel each other out, the thread of relationship between the incidence of ulcer and the consumption of refined protein-stripped carbohydrates runs unbroken through all of them, just as it was shown to do in the preceding section on the geographical incidence.
VII. Various Further Considerations
Before attempting to demonstrate a remarkable correlation between the incidence of peptic ulcer in these Japanese prisoners-of-war and that in the German army on the Eastern Front, certain special features of the disease call for a brief survey here.
Duodenal Ulcer and Gastric Ulcer
Since the first part of the stomach, being the place where the hydrochloric acid is actually secreted, is evolutionarily adapted to the impact of unbuffered acid, whereas the more distant duodenum is adapted only to the impact of acid buffered by the food, the impact of acid insufficiently buffered by refined carbohydrates will chiefly be felt in the duodenum — and in the first part of that structure, since the remainder benefits from the alkaline efflux of the pancreatic juice. The present conception, therefore, sites peptic ulcer normally in the duodenum, and it is highly significant that duodenal ulcer, now so common, is a relatively new disease, [18] hardly occurring before the beginning of the present century — at which time, as will be seen in the curve drawn in Fig. 1 (Chapter II), the rise in the consumption of sugar reached substantially its present exalted level.
The present conception sites peptic ulcer in the stomach itself only when there is gastric stasis, since, in the presence of insufficiently buffered acid, any delay in the gastric emptying-time must, by prolonging exposure to the acid, increase the danger to the stomach, and, by allowing greater backward diffusion of the alkaline pancreatic efflux, decrease the danger to the duodenum. It is therefore logical, on this conception, that gastric ulcer should occur (as it does do) most commonly in: (a) elderly people; (b) frail women; and (c) ill people, since in all these cases there is liable to be hypotonia and gastric stasis. [19] It is also consistent that if there is both a gastric and a duodenal ulcer, then almost invariably the duodenal ulcer precedes in time the gastric ulcer, the duodenal ulcer causing spasm or stenosis and hence stasis in the stomach itself. [20]
The importance of gastric stasis in siting the ulcer in the stomach is also well seen in the case of those acute gastric ulcers which were notorious in young women during the last century and which during the later years of that century disappeared so mysteriously. There seems no doubt that this siting was related to the tight corseting that occurred in those days, which caused actual post-mortem grooving of the stomach by the vertebral column, and consequently very considerable stasis in it. [21]
As regards the higher incidence of gastric ulcer in the unskilled labouring classes, the writer is convinced that this is related to the poorer condition of the teeth and of any dental plates in these classes, since defective mastication has a direct effect on the physical texture of the food swallowed, which in its turn has a slowing effect on the gastric emptying time. [22] For a similar reason the appalling state of the teeth in many younger people today (see Chapter V) may be of importance in the siting of an ulcer.
It will be noted that all the foregoing, which is much elaborated in the main work on Peptic Ulcer, refers to the siting of, not the fundamental cause of, peptic ulceration.
Finally, the author cannot agree with a view that gastric and duodenal ulcer have separate causes. To him this is a case where, again, simplicity points to the truth. To make one cause for an ulcer situated towards the near end of the acid-exposed area (i.e., a gastric ulcer), and another cause for an ulcer near the far end of the acid-exposed area (i.e., a duodenal ulcer) would to him represent the negation of simplicity. He believes a single cause can explain both ulcers, based on man’s interference with the natural buffering of the hydrochloric acid, as has been carefully set out.
It is also to be noted that the term ‘gastric ulcer’ can be deceptive, for any ulcer this side of the pyloric valve qualifies as a gastric ulcer. Yet on the present view a gastric ulcer that is juxta-pyloric is not appreciably different from a duodenal ulcer, whereas a gastric ulcer in the fundus would indicate some reason for a marked delay in the emptying time. Similarly, many gastric ulcers have been reported from Japan, but so many of these ulcers are juxta-pyloric that the fact loses much of its interest. [1]
Sclerotic Peptic Ulcer and Perforated Peptic Ulcer
The chronic, sclerotic ulcers that occur in the eaters of rice and manioc, well known in the countries concerned, and the opposite extreme, the acute perforated ulcers so common in Westernized nations, are both readily explained on the present conception. For in the former case the carbohydrates are stripped of only part of their protein, whereas in the latter case, through the heavy consumption of sugar in these Westernized nations, the carbohydrates are often stripped of all of it. This difference must obviously be reflected in the acuteness of the acid attack.
In this connexion it is of the greatest interest that the chronic sclerosing duodenal ulcer, so characteristic of the Indians in the ulcer belt of India, has changed completely in the Indians in Natal. [23] In these, acute perforations are a prominent feature of the disease, which harmonizes perfectly, on the present conception, with their tenfold greater consumption of sugar. Exactly the same change is now taking place in India itself, especially in the towns, coincident with the replacement of ‘cold rice’ with sweet drinks. [24]
Ranges in Gastric Acidity
These ranges have been studied by Vanzart and others [25] in an analysis of 3764 records at the Mayo Clinic, and a summary of their findings may be appreciated from a study of the curves in Fig. 14, reproduced in a modified form from their paper.
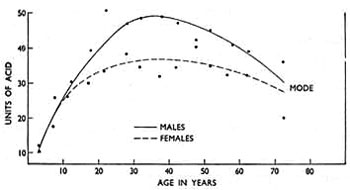 Fig. 14. — Calculated modes of free hydrochloric acid in the stomachs of males and females at different ages. (Modified from ‘Archives of Internal Medicine’.) |
It will be noted that the curve of gastric acidity, starting at a very low level in infancy, climbs steadily all through childhood, and equally in the two sexes; that in the adult it reaches a considerably higher level in the male than in the female; and that subsequently there is a fall in old age, especially in the male, so that the levels in the two sexes again approximate to each other.
In conjunction with these physiological facts it is possible on the present argument to explain further differences in the incidence of peptic ulcer (normally duodenal ulcer). This argument, it will be borne in mind, absolutely excludes the gastric acid as being a primary cause of peptic ulcer, but singles it out as the agent through which the primary cause operates. It thus becomes clear that if the primary cause be present, i.e., interference with the protein in carbohydrate foods and hence with the buffering of the gastric acid, the cause can scarcely become operative at all in infancy, since there is almost no acid to be buffered; that the cause can seldom become operative in childhood, since the curve of acidity climbs but slowly; that the cause in the adult will become operative more easily in men than in women, since the curve of acidity rises considerably higher in them; and that the cause in old age will again become operative less frequently, since the curve of acidity is now falling again. There is thus explained the rarity of peptic ulcer in infancy, its infrequent and equal sex-distribution in childhood, its predilection for men in adult age, and its decline in frequency, and more equal sex-distribution, in old age. Finally, there is also explained the greater incidence of peptic ulcer in those whose natural level of gastric acidity is higher than average.
Heredity
The author has already tried to show that peptic ulcer cannot be due to hereditary defect, and consequently any hereditary characteristics in the disease, which are real, must be those involving the personal make-up of the stomach, duodenum, and other related structures, rendering the people concerned unduly vulnerable to a new environmental factor — such as the one outlined in this work. For example, some of these people are those described in the last sentence of the preceding paragraph.
Against this background the influence of heredity in the causation of peptic ulcer is seen to be of little or no practical importance, since the only thing that is important is the avoidance of the new environmental factor itself For this reason it is considered a waste of time to discuss any hereditary features prominent in persons with peptic ulceration. What help is it to know that a person subject to this disease is liable to have a stomach that secretes much acid, let alone that he belongs to a certain blood group, or for that matter, has ears with well-marked lobes — and that a parent of his had the same characteristics? It is proposed to pass on to something more to the point.
VIII. Peptic Ulcer and the German Army on the Eastern Front
Attention may now be directed to one of the most remarkable facts in the whole epidemiology of peptic ulceration — the near disappearance of the disease in the German army before Stalingrad and on the Eastern Front generally. This development appears to be unknown in this country, though appreciated well enough in Germany itself.
Briefly, at the outbreak of war in 1939, peptic ulcer (chiefly duodenal ulcer) was so common in the German army that actual ‘ulcer battalions’ were formed, to enable the sufferers to have special food. This high incidence will occasion no surprise to anyone who has followed the present argument, for on the one hand refined carbohydrates were still in plentiful supply, and on the other hand personal tastes over various foods were necessarily brushed aside when conscripts and reservists entered regimental life, so that many arbitrary meals were consumed (to be described shortly). Later, when these refined carbohydrates became scarcer and the men got more accustomed to army food, the incidence fell considerably, though it never became very low.
It was, therefore, a source of astonishment to the German medical authorities that peptic ulcer in their troops on the Eastern Front became a rare disease, though the incidence rose all the way back, along the supply lines. There are many references on this subject, but they are all marshalled in two masterly papers by H. Glatzel, [26,27] who was himself medical officer of a rocket regiment on this front. Thus, in rear hospitals ulcer cases constituted 3.2 per cent of admissions; in field hospitals nearer the front line they constituted 1.5 per cent; whereas in the front line itself they were almost never seen. Professor Glatzel quotes first-hand interviews in this respect with medical officers of other regiments. One of these medical officers during eighteen months in front of Stalingrad, amongst hundreds of thousands of troops, stated that he hardly saw a case, and that even old ulcer cases kept free from relapse. Other medical officers were of the same opinion. What was so striking to all of them was the difference in this respect between the front line and the lines in the rear.
Since every single factor on the Eastern Front seemed to predispose to ulcer development, such as (1) anxiety, (2) cold, (3) fatigue, (4) ultra-coarse foods, and (5) deficiency in animal protein, the German medical authorities were greatly perplexed. But an explanation based on the food structure, in accordance with the present conception, is at once possible. For it is just here that a remarkable change occurred.
The account of this change begins with the ever-lengthening supply line of the advancing German army, which at Stalingrad reached a point, even as the crow flies, 1250 miles from the homeland, a distance only 250 miles less than that of London from Moscow. At first the food supplies kept pace with demands, but as the Germans were not prepared for a winter campaign, the situation rapidly deteriorated. The roads soon became marshes, or got deeply covered with snow, and munitions were given priority over food, so that the troops were forced to eat whatever local produce they could lay their hands on. At first they were able to use stocks of grain left behind by the Russians, which were consumed in the crudest state, but later the only local food available was that left actually growing in the fields, and this consisted mainly of turnips and potatoes. These were eaten largely uncooked. ‘The turnips were taken out of the earth, and after scarcely being cleaned were eaten raw; and the same was done with the potatoes, after being peeled.’
At this juncture it must be pointed out that the bread in the German army was already pretty coarse (the flour, according to Professor Glatzel, being at least 80 per cent extraction), so that a bigger difference in the nutrition of these troops lay in the fall in the consumption of noodles, made with white flour and consumed in very large amounts, and of sugar and sweets, the latter of which on this front were largely issued before special exertions. That a big total decline in the consumption of refined carbohydrates took place is certain. Thus Professor Glatzel, in answer to the author’s specific further inquiries: ‘It is beyond discussion that the front line troops were supplied with less refined foods than those further back. As I have repeatedly informed you, the nutrition in these troops was much coarser and heavier, because of the difficulties in the supply line.’ (Given in English.)
This fall came as just as big a surprise to old ulcer sufferers themselves as it did to their medical officers. Thus: ‘The patients often wondered at this strange behaviour in their complaint, which in times of peace they used to blame on dietetic indiscretions or the cold, and which now did not materialize, in spite of the consumption of frozen vegetables, sour bread and raw turnips.’ (Die Kranken wundern sich oft genug selbst über dies merkwürdige Verhalten ihrer Beschwerden, die sie von Friedenszeiten her auf “Didtfehler” oder “Erkiiltung” zurückzuführen gewohnt waren und die nun bei gefrorenem Gemüse, naß-saurem Brot und tagelanger Rübenrohkost oder Erbsen-Speck-Suppe völlig fehlen. [From the original paper.])
Meanwhile, on the supply line towards Germany the food of the troops approximated more and more to the normal, and, as already stated, the incidence of ulcer rose correspondingly.
Peptic Ulcer in German Prisoners-of-War
The climax of this whole incidence-story concerns the Germans captured by the Russians and placed in prisoner-of-war camps. This subject is likewise extensively pursued in Professor Glatzel’s papers, and it would appear incontestable that the disease in these prisoners was one of the greatest rarity, as the following extracts reveal.
Thus Zschau, whose reports are based on careful clinical and autopsy studies during captivity, was amazed at the lack of peptic ulceration in the prisoners, and all the other physicians who were captured agreed with him.
Again, Paschlau, after examining in Germany 2000 repatriated prisoners in 1948-50, gave opinion that the coarse foods of Russian captivity, signally lacking in animal protein, had not only not resulted in peptic ulceration but actually appeared to have prevented it, since many older ulcer cases, which remained symptomless during four or five years of captivity, relapsed on return to Germany.
Finally, W. Burgmann, one of the greatest German authorities on this subject, to whom the author was referred by Professor Glatzel, has been kind enough to send the following personal communication (1962):
‘I was a prisoner of war in Russia from 1944 to 1948. In several of the 22 camps in which I was interned I systematically searched for symptoms of peptic ulcer (X-ray examinations not being possible, of course). In other camps I asked the surgeons about ulcer symptoms, including bleeding and perforation. Yet though they were of the ulcer age, I suspected an ulcer only twice amongst many thousands of prisoners — and these two men were not the normal kind of prisoners but belonged to the “camp bourgeoisie” and received better food than we did. After their release many of those who had suffered from typical ulcer trouble before captivity but had been free from it in the Russian camps, relapsed on their return to Germany.
‘In answer to your special questions: Our bread in the Russian camps did not consist of refined flour, but of unrefined wheat, rye, barley or maize, with frequently up to 20 per cent of peas, beans or soya bean. We were fed the Russian way. Cabbage soup played a dominant part — for cabbage is the main vegetable with the Russians. Besides that, we had soups and mashes made from maize, millet, oats, and soya beans. Animal protein was almost completely missing, as we had no milk, cheese, eggs, or meat. The ratio of fat was extremely small. Sugar, if any, 5 g. a day (i.e., 1/5 oz.); later 10-30 g. (i.e., up to 1 oz.).
‘An explanation for this complete lack of a disease under such conditions, normally so widespread amongst German men, I could not find. I should be very grateful if you could let me know any of your own.’ (Given in English.)
To sum up these statements, it is clear that the freedom from peptic ulceration in these prisoners-of-war in Russia, on a diet consisting essentially of unrefined carbohydrates and practically nothing else, ties up perfectly with exactly the same freedom in the prisoners-of-war in Japan, at the other end of Asia, the only difference in the latter case being that the unrefined grain was mainly rice. A more perfect correlation, on the present argument, could not be asked for.
IX. Disregard of the Appetite, and ‘Stress’
It is now proposed to discuss what is considered to be an important aggravating factor in the production of peptic ulcer — the eating of food in the absence of any proper appetite for it. It must be very doubtful whether this unnatural act can ever of itself cause ulceration, but that it is frequently responsible for considerable aggravation of the primary cause, already advanced, appears certain.
The basis of the discussion is the fact that the size and frequency of the peristaltic waves, and therefore the rate of emptying, in the stomach is largely determined by the degree of hunger present. Ivy and Farley, confirming the work of earlier investigators, showed, indeed, that most of a series of human subjects averaged a fall of 40 minutes in the gastric emptying-time in a meal following a 24-hour fast. [28] If, then, a meal is eaten in the absence of hunger, or without any desire for that particular food, peristaltic action is feeble and the passage of the food through the stomach sluggish.
In these circumstances, however, the relatively stagnant food continues to cause a reflex secretion of gastric juice, and as this accumulates it is very likely to regurgitate into the throat, producing the well-known scalding, acid sensation at the back of the mouth.
To sum up, the unnatural act of eating without desire leads to a disjointed action in the stomach, in which the motor function is more impaired than the secretory one.
It is clear that if the essential cause of peptic ulceration lies in insufficient buffering of the gastric acid, through the interference with the protein content of certain foods, then any stasis of the type just described must act as an aggravating factor, through allowing the gastric acidity to act for a longer time. This is especially true in the case of gastric ulcer, the production of which, it will be remembered, is always favoured by the occurrence of stasis.
From his own experience the author is confident that the whole question of hiatus hernia is also very intimately related to this gastric stasis. It will be dealt with in Chapter XI.
Under modern conditions eating without desire is only too likely to take place. As a preamble, it is necessary to emphasize the personal, idiosyncrasy that exists in food consumption, and here it is important that whereas man towards the Arctic Circle is almost purely carnivorous, towards the Equator he may be purely herbivorous (vegetarian). The Eskimo, for example, lives very largely on meat and fish, whereas races near the Equator often subsist mainly on roots, like those of the yam, manioc plant, and sweet potato, and on cereals such as maize and rice. Even so powerful a higher ape as the gorilla is a pure plant-eater. It must be noted, too, that all meat-eating animals are accustomed to isolated big meals, following a kill, whereas plant-eating animals have to eat much more frequently, since their food is much less concentrated.
In conformity with the difference in man’s food supply in these two widely separated regions of the globe, and his necessary evolutionary adaptation thereto, it is clear that there must occur some expression of this difference even between the inhabitants of northern and southern Europe. Consequently, inhabitants of countries like Great Britain, descended as they are from invaders from one or other of these areas, must exhibit some of this difference also. It would be expected, for example, that a person with fair complexion would show a ratio of choice between animal foods and plant foods appreciably different from that shown by a person of dark complexion. The former would be expected to have a distinct liking for meat and not to have ‘a sweet tooth’ and to prefer large, infrequent meals, whereas the latter would be expected to show the opposite tendencies. These personal idiosyncrasies in food consumption are of great importance. ‘One man’s meat is another man’s poison’ is based on biological truth.
Under civilized conditions the delicate individual adjustment just described, between the body and the foods in its natural environment, is likely to be brutally disregarded, so that a person frequently eats food without any real desire for it. He does this, firstly, through arbitrary meals, and secondly, through arbitrary food mixtures.
Arbitrary meals are meals eaten without any great desire, or even without any desire at all, either because the person is not hungry, or because, if he is hungry, he does not fancy that particular food combination. Starting in the nursery, where children’s meals are often dictated by their parents; progressing through boarding school and possibly university hostel, where routine meals are the order of the day; continuing in business or professional life, where in circumstances of anxiety or haste the midday lunch is often ill-desired, whilst, after work, fatigue may similarly affect the desire for the evening meal; and in meals with friends, where politeness takes precedence to taste, a person under modern conditions is very likely to partake of a long succession of these arbitrary meals. Finally, the best example of all is seen in the advice that has so frequently being given to ulcer sufferers, to keep the stomach from getting empty. This advice, which signally disregards the instinct of appetite and is, therefore, correspondingly at variance with the laws of nature, has been based on the view that the gastric acidity is highest in the empty stomach — a view now known to be incorrect. [29] Furthermore, as the stomach empties, so the state of the wall thickens and the mucous protection rises, giving a maximum in the empty stomach. Unless the natural eating-pattern in the persons happens to be one of very frequent, small meals, such advice is seen to be grievously ill-founded.
In other cases arbitrary meals are not imposed on a person in this way, but are taken voluntarily by him, though for an ulterior motive, unconnected with the appetite, such as to avoid ‘waste’.
Turning now to arbitrary food mixtures, these often occur in connexion with fat consumption, perhaps the best example being provided by fried foods. In these a food such as fish or potato is cooked in fat, and therefore becomes largely impregnated with it.
As a result a person, in order to eat fish or potato he wants, may be forced to eat fat he does not want. Even if he is by nature a ‘Jack Sprat who could eat no fat’, he is forced through an arbitrary food mixture to eat the same amount of fat as another person does.
Other good examples of arbitrary food mixtures are chocolate, where sugar is largely combined with fat; cake, where sugar is largely combined with eggs, fats, and flour; and all proprietary food mixtures. In each of these cases (and scores of others that could be added) the combination of foods is made without reference to the personal desires of the eaters of them. (It is considered also that many cases of food allergy may stem from this cause.)
In nature, food mixtures are usually very simple ones — e.g., protein and sugar (or starch) in the plant foods, and protein and fat in the animal foods, and as the protein is almost invariably in short supply, the tongue usually has a relatively simple problem on its hands in deciding what should be eaten in relation to the body’s needs.
In the diet card at the end of this book it will be seen that the whole subject of eating without desire, somewhat complicated in theory, becomes extraordinarily simple in practice, involving as it does merely the blind following of instinct — the instinct of appetite, as long as the instinct is exerted on foods in a simple, unprocessed state. For the moment, however, it will be necessary to see how stress enters the aetiological scene in peptic ulceration, which it does through this very portal of eating without desire.
Stress
Two forms of stress are dealt with in the separate work, but here we need only discuss the anxiety form, and there could be no better introduction to the study of the effects of this form of stress on digestion than to observe the behaviour of a recently captured animal or bird. Neither of these whilst in an agitated state of mind will touch any food. It is as though Nature wishes to draw on reserves and keep the body clear of commitments during periods of danger, even those concerned with nutrition. Gradually, as the days pass and fear diminishes, the animal or bird will begin to eat again. Herein lies the clue to the proper understanding of the subject. If a man labouring under anxiety similarly adjusted his food consumption to his reduced appetite, he would lose weight, but he would not develop a peptic ulcer. Fasting does not produce organic disease.
Under modern conditions, however, a man is unlikely during periods of anxiety to reduce his food consumption very much, however little appetite he has. One reason for this is that in his own house a carefully prepared meal imposes on him some obligation to eat it. Another reason is that he may become alarmed at not eating and will feel he must eat ‘to keep up the strength’. This form of stress, in short, is likely to precipitate a series of typical arbitrary meals.
Stress, therefore, in the sense of anxiety, becomes, through the disregard of appetite in arbitrary meals, and the gastric stasis that results from it, an important aggravating factor in the causation of peptic ulcer (always assuming the presence of the primary cause). In the absence, however, of this disregard of the appetite, stress plays no part whatsoever.
The distinction between the above view of stress and the one normally held today is a vital one, since a person who understands it can endure immeasurable stress and yet never develop a peptic ulcer. Moreover it must be remembered that anxiety is a natural protective state, subserving a definite function. The words of Laertes may be recalled in Hamlet:
And in the morn and liquid dew of youth
Contagious blastments are most imminent.
Be wary then; best safety lies in fear!
The author has italicized the important phrase. Clearly it is a great advantage to anyone to know that as long as he follows natural principles in eating, he may experience as much fear as circumstances dictate without incurring any risk of peptic ulceration whatever.
If, then, stress need never be even secondarily a cause of peptic ulcer, the author hopes already to have shown that it is positively never a primary cause. For no one could ask for situations involving more formidable degrees of stress than those existing during the destruction of Tokyo, or the siege of Stalingrad — where over half a million Germans lost their lives. Yet neither amongst the allied prisoners in the former case, who were nourished on unrefined grains, nor amongst the German soldiers in the latter case, who were subsisting on even coarser carbohydrates, did peptic ulcer ever appear. The racial incidence, and the historical incidence since the turn of the century, likewise exclude stress in this connexion, as stated earlier.
X. Application of the Present Argument to the Prevention and Arrest of Peptic Ulcer
The medical treatment of peptic ulcer, from the evidence set out in this chapter, will now be seen to lie in almost exactly the opposite type of diet to the orthodox diets commonly prescribed in hospitals. These latter diets normally force people to disregard their appetites and keep their stomachs from ever becoming empty, in the mistaken notion that the acidity of the stomach contents is greatest in the empty stomach, whereas in fact it is greatest in the full stomach, during the height of digestion. [29] These diets also induce people to eat refined carbohydrates in the mistaken belief that coarse foods injure the stomach membranes, whereas what injures these membranes is not coarse foods at all but unbuffered acid. In fact natural, coarse foods no more injure the lining membranes of the stomach than they do the lining membranes of the mouth, and, provided they are properly masticated, are, on the contrary, very safe foods, because of their high buffering power.
It is strange that there should be this widespread fear of coarse foods being harmful in the treatment of peptic ulcer, because, quite apart from the evidence to the contrary set out in this work, Horder, Dodds, and Moran [30] in their work on Bread conclude with the following statement:
‘Consumption of 80-85 per cent extraction flour during the war years also brought out a new fact regarding its effects on certain ulcerative states, such as peptic ulcer. It was decided by the special Diets Committee of the Medical Research Council (Drummond) [31] that this flour, far from being harmful in such complaints, did, in fact, hasten the healing process.’
More recent evidence of the value of coarse foods is provided by trials in 1966-7 by F. I. Tovey [32, 33, 34] in Mysore, India. On two tea estates (Davershola and Telapoya) 800 miles apart, where duodenal ulcer is rife, trials with unpolished rice were made in the treatment of such patients. In actual practice, as unpolished rice keeps badly, rice bran was pasteurized (to inactivate the lipase responsible for the bran going rancid) and was then added to cooked polished rice. Forty-five patients were so treated, under the supervision of their medical officers. At the end of 3 months, 21 of the 45 patients reported a sustained improvement and none of the patients was made worse. After 6 months, 9 of the patients had continued taking the bran, though 2 had relapsed (Fig. 15)
 Fig. 15. — Results of treatment of duodenal ulcer with rich bran, (40 g. per day) for 3 months. |
It must, of course, be remembered that as a duodenal ulcer is liable to leave a scarred, impaired mucosal surface, it by no means follows that a removal of the cause would necessarily cure the ulcer. The author himself is surprised, observing the peculiarly chronic, sclerosing type of duodenal ulcer characteristic of India, that so marked an improvement occurred.
* * *
The orthodox diets have collected much criticism, and quite rightly so, since they fail to prevent the sacrifice Of 30,000 stomachs annually in the operating theatres of the United Kingdom alone. [35] (The present volume should perhaps refer to the physiological sacrifice of the stomach by the more modern vagotomy operations, rather than to its anatomical sacrifice by the older gastrectomy operations.) It is, therefore, submitted that there is every reason to change to the diet that Nature herself indicates — the one, in fact, that is followed by the whole of creation, with the exception of civilized man.
This diet may be described as the following of natural instincts on natural foods. Both components of the rule are equally important. Eating natural foods that are not wanted achieves little, and eating unnatural foods that are wanted achieves infinitely less.
The detailed application of these principles is set out on the diet card at the end of this work, and it must be stressed that this diet is applicable to all the dyspepsias, especially the common ‘acid’ type without demonstrable ulcer.
* * *
Though the principles concerned are outlined at the end of this work, as just stated, the careful integration of natural materials with natural desires will involve much more than just reading through a diet card. A few examples of the difficulties that may be encountered will now be given. Thus, the great ulcer diets of the past have nearly always been based on natural protein foods, in the laudable attempt to neutralize the gastric acid; for example, the Salisbury diet relied upon finely chopped raw meat, the Lenharz diet upon raw eggs, and the Sippy diet upon milk. These materials did indeed buffer the gastric acid for a time after each meal, but unless eaten with desire — which could seldom have been the case — they were doomed to have many failures, because as long as the food stagnates in the stomach, the acid will continue to flow.
The author would like to illustrate these things with the simplest and most natural of foods: milk. Though supremely suitable for the treatment of peptic ulcer, milk is not a food that most adults would be thrilled to take very frequently. And if taken when not desired, milk is very likely to ‘lie like a ball on the stomach’, as patients say, for a long time afterwards. And thus to fail. But for many people the picture can be transformed by eating concurrently a ripe banana or two. Indeed, many people who have no love either for bananas or for milk are very happy with them when they are eaten together, as has long been discovered. The same might happen with milk and a very few of the far more concentrated dates. Or the top, creamy portion of a bottle of milk may be found to go very well with a cut-up sharp apple, over which a few granules only of demerara sugar are sprinkled by the finger and thumb. Then, when such milk combinations begin to pall, the interest in meals may be maintained by the eating of poached eggs or steamed fish, together with some boiled potato made attractive by butter and salt to taste. And so onwards, later, to foods such as underdone steaks.
These examples have been carefully set down because success depends upon them, and they involve a reverence for the human body that demands the utmost attention to personal tastes, including the avoidance of any meal at all if the patient is not hungry (as may well be the case, if he is in bed). The use of alkaline drugs for pain will clearly lie in the hands of the physician alone, for to eat food only to stop pain could never be entertained by the author for a moment.
The author can almost hear some of the readers of these paragraphs saying ‘this régime is not practicable’. He has, himself, however, found it perfectly practicable, but would stipulate that in a ward everything depends on the ward sister having the same attitude as that set out here, and on there being a little co-operation in the kitchen.
In connexion with the supreme importance of natural feeding as compared with the ‘stress’ mentioned above, he is tempted to refer, for illustration only, to an episode in his naval experience of many years ago, because some of his readers may themselves be sufferers from dyspepsia or peptic ulcer, and the episode may possibly increase their confidence in the natural approach.
In 1942 the author was Senior Medical Officer of the battleship King George V, stationed at Scapa Flow in the Orkneys and at that time the Flagship of the Home Fleet; and one day the Commander-in-Chief reported with symptoms of duodenal ulcer, from which he had suffered many years previously. A barium-meal examination was arranged in H.M. Hospital Ship Amarapoora, and the films showed an unmistakable duodenal ulcer, about the size of the little finger-nail. The Admiral resisted our desire to send him to hospital; he said the German battleship Bismarck was at that moment about to break out into the Atlantic, and that this was clearly a very difficult time for him to leave the ship. The situation was one of great anxiety to everyone, including the author and his junior colleague, the present Dr. R. I. G. Coupland, especially as the raw materials so vital in the treatment just set out, such as fresh milk, fresh cream, fresh fruit, and fresh meat of high quality, were hard to come by at sea in wartime. However, a stock of fresh milk and fresh cream was hastily scraped together locally, before leaving Scapa; and some days later, during refuelling in Iceland, the author was provided with transport and allowed to travel to the capital, Reykjavik, to replace and extend the range of materials, including the purchase of fresh cream, steaks, and some fresh fruit. During the whole of the period now under review, amounting to some ten days, the Commander-in-Chief was given these natural foods of high quality, and, what is of crucial importance, he greatly liked eating them. He was also given some magnesium trisilicate for pain at night, but little of this was needed later. At the end of the period, which had been one of the greatest possible stress and anxiety to him, involving as it did his constant presence on the bridge, and during which occurred the loss of our battle-cruiser Hood, the destruction of the Bismarck, and the cutting in two by tragic mishap of our own attendant destroyer, the ship arrived at Rosyth, in the south of Scotland. The Admiral had by then lost his symptoms, and a fresh X-ray examination revealed that the ulcer had healed over in spite of all the turmoil — but with sugar and white flour sedulously excluded.
Success with the natural approach cannot, however, be expected in advanced cases of peptic ulceration, with much scarring of the mucosa. Recourse must then be had to surgery, just as dental decay, certainly preventable though it is, needs skilled dentistry once it has arrived, as has been stated elsewhere in this work.
The author has always found that the natural approach to the treatment of peptic ulcer, as set out in the diet card referred to, is immensely rewarding, but it demands the personal supervision of the physician himself, the understanding and co-operation of the patient, and the availability of some of the natural foods which are so necessary. The last, alas! implies that the patient’s means should be somewhat above the lowest. Any routine application of this approach in a hospital out-patients’ department could make a shambles of the whole subject.
Finally, the author cannot, himself, see any future in the use of drugs (e.g., carbenoxolone) for the long-term alleviation of peptic ulcer, for they cannot remove what he considers to be the essential cause of the condition.
References
1. Cleave, T. L. (1962), Peptic Ulcer. Bristol: Wright. (U.S.A. The Williams & Wilkins Co., Baltimore.)
2. Lancet (1959), 1, 1107.
3. Doll, W. R. S., Jones, F. Avery, and Buckatzsch, M. M. (1950), Spec. Rep. Ser. Med. Res. Coun., Lond., No. 276.
4. Based on McCance, R. A., and Widdowson, E. M. (1960), The Chemical Composition of Foods, 3rd ed. London: H.M.S.O.
5. Neilsen, N. A., and Christiansen, H. (1932), Acta Radiol., Stockh., 13, 678.
6. Tovey, F. I., quoted by Cleave, T. L. (1962), Peptic Ulcer, 134. Bristol: Wright. (Further paper awaiting publication.)
7. McCance, R. A., Prior, K. M., and Widdowson, E. M. (1953), Brit. J. of Nutrit., 7, 98.
8. Lennard-Jones, J. E., Fletcher, J., and Shaw, D. G. (1968), Gut, 9, 177.
9. Kirschner, A. A. (1944), Rev. Gastroent., 11, 397.
10. Dogra, J. R. (1940), Indian J. Med. Res., 28, 2; and (1941), Ibid., 29, 665.
11. Aykroyd, W. R. (194O), Indian Med. Res., Mem., No. 32.
12. Konstam, P. G. (1959), Indian J. Med. Sci., 13, 486.
13. — (1958), Schweiz. Z. Alg. Path., 2, 229.
14. Kouwenaar, W. (1930), Ned. T. Geneesh, 49, 2321.
15. Cleave, H. L. (1958), J. R. Nav. Med. Serv., 44, 77.
16. Illingworth, C. F. W., Scow, L. D. W., and Jamieson, R. A. (1944), Brit. Med. J., 2, 617, 655.
17. Report on Nutritional Survey in Netherlands East Indies (1948). The Hague: Netherlands Red Cross Society.
18. Beckett, E. M. (1960), in Peptic Ulceration (ed. Wells and Kyle), 2. Edinburgh: Livingstone.
19. Jones, F. Avery (1957), Brit. Med. J., 1, 719, 786.
20. Johnson, H. Daintree (1955), Lancet, 1, 266.
21. — (1957), Ibid., 2, 515.
22. London, E. S. (1925), Experimentelle Physiologie und Pathologie der Verdauung, 52. Berlin: Urban & Schwarzenberg.
23. Cleave, T. L., Campbell, G. D., and Painter, N. S. (1969), Diabetes, Coronary Thrombosis, and the Saccharine Disease, 2nd ed., 99. Bristol: Wright.
24. Madanagopalan, N., Subramaniam, R., and Krishnan, M. N. (1968), Gut, 9, 69.
25. Vanzart, F. R., and others (1932), Arch. Intern. Med., 49, 345.
26. Glatzel, H. (1945), Ergelm. Inn. Med. Kinderheilk., 65, 504.
27. — (1952), Arztl. Wschr., 7, 1063.
28. Ivy, A. C., and Farley, G. B. (1929), Amer J. Physiol., 91, 205.
29. Atkinson, M., and Henley, K. S. (1955), Clin. Sci., 14, 1.
30. Horder, Lord, Dodds, Sir Charles, and Moran, Lord (1954), Bread, 179. London: Constable.
31. Drummond, J. C. (1947), ‘Nutritive Value of Bread’, Sanderson Wells Lecture, Middlesex Hospital.
32. Tovey, F. I. (1972), Trop. Geogr. Med., 24, 107.
33. — (1972), J. Christian Med. Assoc. of India, 47, 314.
34. — (1972), Brit. Med. J., 2, 532.
35. Stammers, F. A. R. (1961), Brit. J. Surg., 49, 28.
Chapter XI
A Different Type of Over-Consumption, that is Not Specifically Due to the Taking of Refined Carbohydrates
Simple Hypertension. Gout. Hiatus Hernia. Acne Rosacea
ALTHOUGH the taking of refined carbohydrates is by far the most important cause of over-consumption, as has been set out in this work, it is not the only cause. Another cause lies in the common occurrence of people eating when they are not hungry, and the conditions that this leads to are not in the author’s opinion basically manifestations of the saccharine disease.
The important question of eating in the absence of hunger has been carefully described in Chapter X, on peptic ulcer, and of the examples set out there perhaps the best is seen when people eat in the company of others, especially if this is attended by the taking of alcohol. One is reminded of the huge meals, accompanied by the drinking of large quantities of port, that took place in past generations, as in the times of the earlier Georges. But there is no need to go back to these extreme examples; the fact is that even today in communal feeding a great deal of food is eaten chiefly because it is there, or for an ulterior motive not connected with the appetite as, for example, in many businessmen’s lunches.
Simple Hypertension and Gout
The apoplexy and gout so commonly recorded amongst earlier generations (‘our forefathers used to chalk their billiard cues with the knuckles of their fingers’) were certainly not basically caused by the consumption of refined carbohydrates, which, as we have seen, was enormously less then than now. Nor has there been any explosive rise in the incidence of apoplexy and gout since the end of the past century, which has been so typical of appendicitis, peptic ulcer, coronary thrombosis, and other saccharine manifestations. It has also to be remembered that refined carbohydrate foods undergo a relatively complete combustion in the body compared with protein foods like meat, fish, and eggs. They therefore leave little work for the kidney to do in excreting metabolic end-products, and so would not be expected to lead to undue wear in that organ, which wear plays a part even in simple hypertension. Nor, as regards gout, are they of themselves heavy direct producers of uric acid in the way that protein foods are.
The author has not therefore included simple hypertension and gout as basically saccharine conditions. He considers they are essentially caused by the type of over-consumption set out above, however much this is aggravated by the other type of over-consumption (from taking refined carbohydrates). He is well aware that amongst primitive peoples, on a very simple, natural diet, these conditions are rare, but that is equivocal as regards the basic causation, for eating without hunger is rare in them too.
Hiatus Hernia
Another condition considered here to be due to over-consumption through disregard of the appetite — eating in the absence of hunger for what is eaten — is the ordinary sliding hiatus hernia. As was stated in Chapter X, physiologists have shown that the emptying time of the stomach is largely determined by the degree of hunger present when the meal is eaten, and, as the author has pointed out elsewhere, [1, 2] just as the oesophageal sphincter contracts strongly in a fast emptying time, so it will relax in a sluggish one. And it is this relaxation that the author submits allows the oesophageal reflux (‘acid eructations’ and ‘heartburn’) that initiates, and is always the hallmarked symptom of, hiatus hernia.
The author reached the above conclusion over hiatus hernia through considerations of natural principles and through many years’ practice in naval hospitals, where the dyspeptic symptoms of acid eructations and heartburn were commonly encountered. The reason for the commonness of these acid eructations in the Navy lay, in his opinion, in the eating without hunger likely to occur in life at sea, with communal routine meals on the one hand and frequently restricted exercise in ships on the other. (Hiatus hernia itself is, however, seldom seen in the Navy, since the majority of ratings leave the Service at the age of 40 — i.e., many years before hiatus hernia often presents itself clinically.)
He learnt that the alleviation of reflux unquestionably lies in teaching the patient only to eat when he is hungry — including hungry for that particular food. [Hunger by itself, but not for that particular food, is not so relevant. Thus, a skilfully cooked pork chop, considered a difficult food to digest, will, if eaten with real hunger for it, become like a ship sunk without trace; whereas a pint of milk, considered an easy food to digest, will, if taken without hunger for it, ‘lie like a ball on the stomach’ for an hour or two afterwards and cause abundant eructations.] In connexion with eating only in the presence of hunger, it is always more accurate to make this decision before going to the table, as set out in the diet card at the end of this work.
The author therefore contends that hiatus hernia is secondary to chronic oesophageal reflux — i.e., it is the result of reflux, not the cause of it. This contention of the author’s, reached by natural considerations and clinical experience, has received support from a very different angle — a surgical one. K. S. Mullard, [3] as the result of surgical experience comprising over 700 operations for this condition, has come to the conclusion, as he has stated in his Hunterian lecture on the subject, that hiatus hernia is in most cases primarily a functional, not an anatomical, condition, and has directly supported [4] the author’s contention above.
As regards the actual mechanism of production of sliding hiatus hernia (which is so much less important than the cause, as advanced above), the author has always considered that the reflux produces intermittent (and therefore not radiologically easily demonstrable) enlargement of the oesophagus, with consequent enlargement of the hiatus in the diaphragm. This has very recently been shown to be quite possible. [5] Alternatively, the unnatural act of eating without true hunger could upset the tonal balance between the circular muscle in the oesophagal sphincter and the longitudinal muscle in the oesophagal wall, for K. S. Mullard [3] has shown how big a part this latter muscle plays, through pulling up the oesophagus and proximal part of the stomach, in the production of a sliding hiatus hernia.
Whichever mechanism was proved right (and the first is far the simpler), it would be essential to realize, as already said, that eating without hunger can only really be revealed by consulting the appetite before going near the table. From his experience, also, the author is confident that acid eructations are often a far more delicate indication of reflux than is retrosternal pain (heartburn).
The author cannot support that straining at stool plays any part in the causation of hiatus hernia. [6] In the first place, if this were the case the condition would be expected to be associated with other hernias, [7] and with chest conditions causing chronic cough, but this is not the case, though reflux can itself cause some inhalation-infections in older people. And in the second place, in his experience, regulation of the bowel, including by unprocessed bran, makes no difference whatever to the occurrence of the eructations (reflux).
Before leaving the subject of oesophageal reflux, it is worth noting that any acid eructations occurring through the above mechanism are always at their most acid after the eating of concentrated sweetstuffs. This is because there is nothing in such foods to neutralize the gastric acid, as explained in Chapter X, on peptic ulcer. Therefore, though such foods do not provide the mechanism, they aggravate its effects. Sweetstuffs, it is hoped, would largely be avoided by readers of this work, but very acid eructations may follow the taking of even such a natural food as dates — though it will be remembered (Chapter X) that these concentrated fruits are not natural to the white races. If, therefore, white people eat a concentrated fruit like dates, they will be wise to take them with a glass or more of milk, with which they form a delightful combination. The same is true in many cases even of the less concentrated banana.
Finally, hiatus hernia does not occur amongst non-Westernized peoples, as has recently been cogently set out by D. P. Burkitt and P. A. James, [8] but as in the case of hypertension and gout, described above, this is equivocal as regards the mechanism of causation. So is the frequent co-existence of obesity.
Acne Rosacea
In the author’s opinion acne rosacea is also related to acid eructations, through their producing a reflex flushing of the skin over the nose and cheeks. This effect is magnified if the regurgitations are unduly irritant, as from imperfectly buffered gastric acid, as he has set out in his work on Peptic Ulcer, or from strong alcohol, hot tea, etc. Certainly he has found that this distressing complaint can be alleviated by the avoidance of eating in the absence of hunger, and of drinking cups of hot tea, and glasses of alcohol, both of which are normally taken without any relationship to hunger whatever.
References
1. Cleave, T. L., Campbell, G. D., and Painter, N. S. (1969), Diabetes, Coronary Thrombosis, and the Saccharine Disease, 2nd ed. Bristol: Wright.
2. Cleave, T. L. (1971), Brit. Med. J., 4, 50
3. Mullard, K. S. (1972), Ann. R. Coll. Surg. Eng., 50, 73.
4. — (1971), Brit. Med. J., 4, 236.
5. Wolf, B. S. (1973), Am. J. Roentgenol., 117, No. 2, 231.
6. Cleave, T. L. (1973), Lancet, 2, 268.
7. Mullard, K. S. (1973), Ibid., 2, 451.
8. Burkitt, D. P., and James, P. A. (1973), Ibid., 2, 128.
Chapter XII
Conclusion
THE conception presented in this work, based on evolutionary, epidemiological and other scientific considerations, recalls the conclusions that many have arrived at instinctively in the past, without any scientific aid at all. Thus Horace, some 2000 years ago, as stated at the very beginning of this book, warned that ‘you may drive out Nature with a pitchfork, but she will ever hurry back, to triumph in stealth over your foolish contempt’.
In much more recent times eminent members of our profession, such as Sir Robert McCarrison, have pursued a similar approach, based on natural considerations, and the thirty-two practising physicians and surgeons [1] in the county of Cheshire — who played no small part in founding the present Soil Association in this country, dedicated to natural principles in nutrition and in agriculture — have laboured tirelessly in the same vein, and in particular have blamed the spate of modem degenerative diseases on alterations in our food, and urged the medical profession to return to the Hippocratic view — that the physician should also be a naturalist and should take cognizance of the cycle of Nature as well as of man. These beliefs were carried further forwards in 1957 by over 400 doctors and dentists. [2]
The dental profession has always been the most aware of the impact of refined carbohydrates, the effects of which on the teeth smite the eye, and a member of that profession, Mr. Weston Price, [3] made one of the most revealing of all personal epidemiological studies. He travelled purposefully in different parts of the world and found that wherever a civilized, refined diet overtook an erstwhile healthy race, dental decay became rampant. He also showed that from a very early age the skull itself sometimes shared in these effects, and from this observation made penetrating suggestions concerning delinquency.
It is pertinent here to observe that it is the Medical Officers of Health in this country who, more than any other group, hold in their hands the practical application of the dietetic principles set out in this work. From this fraternity the author has received no greater support or more information than from Dr. Kenneth Vickery, who since the mid-1950’s has written repeatedly of the dangers of refined carbohydrate foods in human nutrition, especially in connexion with the giving of cane-sugar in milk feeds to babies, and the ever-earlier introduction of refined farinaceous foods into the diet of infants. He has considered that such additions not only are the direct cause of dental decay and ever-more-frequent obesity in young children, but also probably lay the foundation for other conditions in later life, such as coronary thrombosis.
While lending sustained and influential support to the conception of the saccharine disease, Dr. Vickery has criticized the author for not including more prominently in this disease the vitamin deficiencies that stem from refined carbohydrates, to which some allusion has been made. This criticism is only too valid, especially since, as Dr. Vickery has pointed out, such deficiencies must be accentuated in many sufferers from the saccharine disease who are obese, since in them the vitamin claims of much non-vital tissue (fat) are in conflict with the claims of tissues that are very vital indeed. In old age, too, as stated earlier, Dr. Geoffrey Taylor and others have shown how serious these deficiencies can be, partly through ignorance of the foods needed, partly through lack of money to buy such foods, and partly through lack of energy to forage for them even if there is the money to buy them.
These vitamin deficiencies, however, though a formidable public health problem, are relatively well understood, and in a skeletal work of this sort the author has preferred to devote the space to conditions where he may have something to contribute. But Dr. Vickery’s points are very real ones. One thing that seems to be very clear is that vitamins should always be taken, if that is remotely possible, in their natural setting, i.e., in the natural foods containing them. By this means not only are there taken any vitamins that have not yet been isolated, but also there is avoided the risk of overdosage, which can at times be just as dangerous as underdosage.
Meanwhile, in a recent personal communication (January, 1973), which the author is privileged to quote, Dr. Vickery states that he is entirely certain that ‘if the present conception becomes applied to public health, it will not only result in a dramatic reduction in the degenerative diseases of today and in the personal suffering caused by them, but will also bring a corresponding relief to the overburdened resources of the National Health Service’.
In this connexion Dr. Vickery, together with the author himself, would single out one step which appears to be eminently feasible right away — a campaign to persuade people to change to a true wholemeal bread, coupled with the elimination of white bread and refined farinaceous products from the dietary of hospitals and other public institutions. The provision of unprocessed bran on a large scale, for the millions of sufferers here from ordinary constipation, would appear to be the thin end of the wedge in this respect. Another feasible step — but much less feasible, alas! — would be a modification of the contents of school tuckshops, so that sweets were replaced by such things as raw fruits, dried fruits, and nuts, in order that some inroads were made on the present dreadful commitment to sweets by the young people in this country. Such a step would have to make up any financial loss to the shops concerned — the cost of which would come back many times over in the accounts of the National Health Service. A very similar step would be desirable in hospital canteens, too, where at the moment are available only the foods that are responsible, if this volume counts for anything, for so many of the patients being where they are.
A Note on Treatments
The present work is essentially one on aetiology, but since the first step in the treatment of a disease lies in removal of the cause, where this is possible, the work also becomes implicated in treatment. And here a note of caution is necessary. For the natural approach in the quest for causation, as discussed above, does not always lead to a natural approach in treatment, too.
Thus, as suggested earlier, [4] it is possible to divide all diseases into, as it were, unnatural and natural groups. The members of the unnatural group, confined to civilized man and some domestic animals, include the degenerative conditions dealt with in this book; per contra, the chief members of the natural group, seen in all living creatures, include the infections and infestations, where one organism preys upon another in the struggle for existence — good examples of which in humanity are attacks by viruses, by bacteria, and by multicellular organisms like a tapeworm or, for that matter, a tiger.
Sometimes the distinction between unnatural and natural diseases becomes blurred, but, as a rule, the absence or presence of infectiousness (either direct or, as in the case of malaria, indirect) decides the issue, for only by infectiousness can the natural diseases continue occurring from generation to generation. This test readily reveals the difference between an unnatural disease like appendicitis and a natural one like typhoid fever.
Here the following extract from the author’s original paper [4] is relevant:
‘At this stage one might refer to the light thrown on this classification of diseases by some consideration of the diseases that occur in animals. A perusal of some of the textbooks of veterinary surgery is not only a very interesting experience, but it confers added perspective on the nature of disease that is most valuable.
‘In surveying such a panorama of disease it becomes very clear that the dog assumes a position in relation to other animals very similar to that occupied by civilized man in relation to other, primitive races.
‘In modern conditions the dog, which in Nature is almost a pure carnivore, has largely been turned into a herbivore. In Nature, as in an English countryside, it would spend its time catching rabbits, rats, and other similar mammals, and would never turn aside to eat the ears of the wheat ripening in the field. ‘The nearest it would get to that would be occasionally to make itself sick by eating a few blades of grass. Yet in civilized conditions, especially in those of poverty, the dog lives on wheat, in the form of bread, dog biscuits, and related foods, to a much greater extent than it does on flesh. Meat and fat are expensive foods; bread is a cheap food; it is not surprising, therefore, that most dogs in English homes live on a preponderance of farinaceous, as opposed to protein, materials.
‘This results in the dog being exposed to all the unfortunate consequences of an over-consumption of carbohydrates that have been mentioned earlier in the case of civilized man. Thus the dog suffers from dental caries, diabetes, chronic interstitial nephritis and so on; and no doubt if dogs were more carefully examined in the last stages of their lives, these conditions would be found still more frequently.
‘Although tumours will not be dealt with in these pages, it is interesting to quote from Hamilton Kirk: [5] “Tumours in dogs are very commonly found, but in cats much less so. ‘The malignant variety is, unfortunately, very prevalent; in fact, cancer may be said to be quite common.” (This subject has recently been elaborated in The Lancet. [6])
‘But all the above diseases are rarer in the cat. Why? Because the cat, also a pure carnivore, differs in its food habits from the dog, under domestic conditions. Although it lives with humanity, “it walks alone”, and avoids most of the food eaten by the dog. It lives on milk, fish, mice, birds, and so on, rather than on biscuits. The carnivorous cat, in short, under civilized conditions, largely stays carnivorous. And that is the obvious explanation why the diseases of civilization are more rarely seen in it.
‘Consideration of such facts as these from the case of animals makes the classification of diseases into two main groups, the natural and the unnatural, even more easily appreciated, perhaps, in the sister science of veterinary surgery than in that of medicine itself.’
Now, the treatments in these two groups of diseases are diametrically opposite to each other. For in the unnatural diseases the natural approach in treatment is correct, mainly consisting as it does in the removal of unnatural causes. It is here that the diet card at the end of this work comes into its own. But how relatively ineffective is this approach in the natural diseases! Of what avail are the hands in an attack by a tiger? A revolver is more to the point. And, indeed, in the natural diseases generally, such as the infections and infestations, highly unnatural treatments are indicated, including the use of drugs, antibiotics, and surgical operations.
Such steps are also needed even in the unnatural diseases for any damage already sustained. For example, the natural diet will certainly prevent and arrest dental decay, but for any decay already present normal dental treatment will be imperative. Similarly, in diabetes the natural diet will prevent and may well arrest the disease, but it can never replace the use of insulin where the damage already sustained indicates the need for this material; and likewise over operative treatment in appendicitis.
It is seen that controlled and co-ordinated naturopathy, especially in the reverence it betokens for the human body, is a very valuable approach in therapeutics, but its blanket application to disease generally would be totally unjustified.
The Outlook
Since this is mainly a work on the causation of disease, it is not really implicated in what civilized man in general, and Westernized man in particular, will do about such causation, if it becomes generally accepted as true. This is an entirely different subject, just as the discovery of smoking as the main cause of lung cancer, and what the public does about it, are two subjects that are entirely different from each other. If the author were asked what he thought the public will do in the present case, over the consumption of refined carbohydrates, he would hazard the guess: in prevention, very little; in treatment, quite a lot; in short, people will go on enjoying themselves till they get hurt. This would follow the smoking and lung cancer precedent, though in the present case a drug habit is not involved, and so the outlook may be brighter.
But at this point the question of economics comes into the picture. For if it were just a question of substituting unrefined carbohydrates for refined ones, little loss of pleasure would be involved and therefore little opposition would be expected. But such a step involves some extra expense, and the more people who attempt such substitution, the greater the expense becomes, owing to the ensuing rise in prices, especially of raw fruit. This is why the author singled out the eating of wholemeal bread as the first and most feasible step, and even here there could eventually be considerable repercussions in the animal-feed industry.
It may well be, in fact, that the struggle for existence, in the shape of simple economics, will compel humanity to adapt itself to the consumption of these refined foods. But this adaptation will take many thousands of years and will be accompanied by immense personal suffering. For those not wishing themselves to participate in this grim evolutionary event, and who are prepared to spend a little more money, the diet card, already mentioned, will, if the author’s experience is any guide, prove to be valuable. It is in a form suitable for the lay public and saves a great deal of talking and explaining on the part of medical practitioners.
In conclusion, the author hopes that the lack of academic detail in this work will not be construed as a weakness. Were it so construed, he would try to defend himself with the following: In many of the conditions set out here as parts of a single master-disease, mostly erupting within the past 100 years, particularly such conditions as colonic stasis (with its diverticular and venous complications) and extending through the Escherichia coli infections, peptic ulcer and diabetes right up to the dreaded coronary thrombosis, what have the thousands of highly academic papers published on these conditions so far achieved? They have produced miraculous surgical and pharmacological antidotes to the ravages produced by these conditions on the human body, but the conditions have not been stopped from occurring; on the contrary they are commoner now than they ever were, and most of them are still getting commoner. Nor have members of our own profession been in any way absent from the sufferers in this remorseless advance. May not the author therefore plead, with all humility, that there may be room for a different type of work, embodying a much greater reverence for Nature herself? — a work where academic details that do not seem vital are deliberately omitted in the interests of greater perspective and simpler conclusions. And with this reference to simplicity he ends his book on the same note as that on which he began it.
References
1. Cheshire Panel Committee (1939), Brit. Med. J., 1, suppl., 157.
2. Lancet (1957), 1, 152.
3. Price, W. A. (1950), Nutrition and Physical Degeneration. Los Angeles: American Academy of Applied Nutrition.
4. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 40, No. 2, 55.
5. Kirk, Hamilton (1945), Index of Diagnosis, 42, 449-50. London: Baillière, Tindall & Cox.
6. Leader (1968), Lancet, 2, 618.
Chapter XII
Appendix
Originally published in Peptic Ulcer by T. L. Cleave. Bristol: Wright (1962).
THOSE who consider that small alterations in the natural environment can be ignored should study carefully a disaster like that of acute bloat in cattle. In this condition a great accumulation of uneructated gas occurs in the fourth stomach or rumen of ruminants, especially cattle. It is a common and serious problem in animal husbandry, and carries a high mortality (15-100 per cent). [1] The cause of acute bloat lies in an insufficient amount of fibre in the diet, usually due to allowing animals to graze on grass having too high a proportion of clover, which contains relatively little fibre. This lack of fibre leads to insufficient stimulation of the stomach musculature, and so accumulating gas is not eructated. The rumen becomes, therefore, distended to a dangerous degree, and the animal frequently dies.
Grass and clover are both natural foods for cattle, but in a natural environment grass would never have such a high proportion of clover; this is achieved in farming today by ploughing up the land and sowing a suitable seed mixture. It must always be a source of amazement — and of instruction — that so large and powerful an animal as an ox can rapidly be killed by such a trifling alteration in its natural environment. When it is remembered that today mankind commonly alters its natural environment by many times this extent, in removing some 30 per cent of its substance from his grain and 90 per cent from his sugar-beet and sugar-cane, it must engender profound scepticism in any thinking person that he can be a party to these practices and get away with them. In particular, the greatest reserve should be exercised in dismissing any known effects of these practices on stomach function just because the effects appear to be small.
Reference
1. Menzies, D. W. (1952), Bloat and the Bloat Survey. British Veterinary Publication No. 23. London: British Veterinary Association.
The Natural Diet for Health
Guide for the Prevention and Arrest of All the Manifestations of the Saccharine Disease
Preliminary
THE word ‘saccharine’, which means ‘related to sugar’, is pronounced like the river Rhine, which sharply distinguishes it from the word for the chemical sweetener. The starch in flour is digested in the body into sugar, and the word ‘saccharine’, as used here, means related to white flour as well as to white or brown sugar; and the term ‘saccharine disease’ covers all the conditions held to be due to the consumption of these two artificially refined carbohydrate foods. The saccharine disease includes dental decay and pyorrhoea; gastric and duodenal ulcer and other forms of indigestion; obesity, diabetes, and coronary disease; constipation, with its complications of varicose veins and haemorrhoids; and primary Escherichia coli infections, like appendicitis, cholecystitis (with or without gall-stones), and primary infections of the urinary tract. The same applies to certain skin conditions. Not one of these diseases is for practical purposes ever seen in races who do not consume refined carbohydrates.
The simple instructions in this card thus prohibit white flour and sugar, but permit natural bread and natural sweet things (and also nearly every other type of foodstuff). By this means the diet is reduced to the evolutionary level to which man is adapted and reflects the principles of natural feeding seen in all living organisms. That is why this card is entitled ‘The Natural Diet for Health’, since the diet concerned is not really a medical diet at all. For the same reason it is not harsh, nor is it liable to change.
Needless to say, although the diet is aimed at the prevention and arrest of all the conditions listed above, other medical measures may be indicated for damage already inflicted by the consumption of these refined foods. For example, the prevention of dental decay will not reduce the necessity of dental treatment for decay already present.
Rules
The diet is based on two rules only, which may be summarized as follows:
1. Do not eat any food unless you definitely want it
Eating food that is not wanted is a most unnatural act, yet frequently takes place today. One reason lies in eating routinely, especially when one is overtired or worried and does not really fancy any food at the time; another reason lies in eating a meal because someone has taken the trouble to prepare it, or in eating food to avoid wasting it; whilst yet another reason lies in eating food on social or business occasions, when it is taken for motives of politeness or policy. On all these occasions ‘if you don’t want it, don’t eat it’. This decision is always made most accurately before coming to the table.
2. Avoid eating white flour and white or brown sugar
This means avoiding on the one hand white bread, pastry, cakes, biscuits and other confectionery; and on the other hand white or brown sugar, jams, ices, chocolates, sweets, and sweet drinks. Substitute a true wholemeal bread and wholemeal flour for the first group, and raw or dried fruit for the second group. This restores the natural fibre to the diet, which will now be shown to be of the greatest importance. Notes on the application of this rule will be given later.
How These Two Rules Prevent Disease
Dental Decay and Pyorrhoea
The removal of coarse fibre in the manufacture of white flour and sugar prevents the natural cleansing of the teeth, and hardening of the gums, which take place when the unrefined original foods are consumed. The shocking loss of teeth from these causes today, even in the very young, is most certainly preventable.
Gastric and Duodenal Ulcer
In treating these and other forms of indigestion the aim should be to prevent an excess of acid forming in the stomach, which is the main cause of the trouble, and not to neutralize the excess of acid with alkaline drugs (except in the presence of actual pain, under medical supervision).
There are two unnatural factors in the production of this excess acid, and both must be removed. One factor is eating food that is not wanted. Under these circumstances the food stagnates in the stomach and excess acidity results, which can often be felt at the back of the throat. Rule 1 is therefore most important, especially in times of worry. Note also that this rule prohibits the taking of unwanted food merely to relieve gastric pain. It is true that food may temporarily relieve such pain, but this unnatural food intake is not the right answer. Pain calls for alkaline drugs, under medical supervision, and probably treatment in bed.
The other factor in the production of excess acidity is the eating of white flour, or sugar. In the refining processes employed in the manufacture of these substances the protein component in the wheat is considerably reduced, and in the sugar-cane and sugar-beet is removed altogether. Since protein is the only foodstuff that neutralizes the gastric acid, the eating of white flour or sugar exposes the stomach membranes to an unnaturally fierce attack by the gastric acid, which may result in an ulcer. In places like India and Japan the refining of the rice leads to even more ulceration than occurs in this country. Hence the importance of the second rule set out above.
Obesity (Overweight)
Obesity stems from the appetite being deceived by the unnatural concentration present in white flour and in sugar, so that a person eats too much. For example, the average consumption of sugar today is about 5 oz. per head per day (against less than 1 oz. about a century ago). This 5 oz. is contained in nearly 3 lb. of sugar-beet or in up to a score of ordinary apples. Who would consume this quantity of sugar in its natural, dilute form? The same argument applies to white bread, and other articles containing white flour, as compared with unrefined wholemeal bread.
By following Rule 2, above, the natural fibre (roughage) is restored to the diet, and the natural dilution is restored also. As a result the appetite can again be allowed to regulate the amount to be eaten, as it is designed to do, and we can ignore any question of calories, just as all creatures in the wild state ignore them (and they never suffer from overweight).
For the removal of overweight already present, a certain amount of starvation may be necessary, as in the omission of breakfast and afternoon tea — to be done under medical supervision.
No forced exercise is advised in obesity.
Diabetes and Coronary Disease
The causation of these conditions is likewise connected with over-eating, through the appetite being deceived by concentration in the food, and the same unrefined diet is indicated. Any other treatment must be under medical supervision.
Simple Constipation, and its Complications of Varicose Veins and Haemorrhoids (Piles)
Simple constipation is caused solely by the removal of fibre (roughage) in the manufacture of white flour and sugar. Varicose veins and haemorrhoids arise from the fact that in constipation the unnatural accumulations in the bowel press on the great veins in the abdomen which are bringing up the blood from the legs (thus causing varicose veins), or on the veins bringing up blood from the back-passage (thus causing haemorrhoids). None of these conditions is seen, even in pregnancy, in native ram who do not consume these refined foods. The basic treatment of all these conditions lies in the restoration of the natural fibre to the diet, as in Rule 2, above.
Primary E. coli Infections
Appendicitis, cholecystitis (inflammation of the gall-bladder, with or without gall-stones), diverticulitis (inflammation of the bowel), and cystitis (inflammation of the bladder) all arise from the hordes of microbes subsisting on unnatural food surpluses in the gut, which result from people eating too much, for the reason given. If this over-consumption is prevented in the basic manner just described, the microbes are starved out. Hardly any of these conditions are seen in those races who do not eat white flour or sugar. In the fully developed acute attack antibiotic treatment and surgical operation may be essential.
Certain Skin Conditions
The bacterial decomposition just described leads to much offensiveness in the motions and in any wind that is passed. These offensive products when absorbed into the bloodstream may be responsible for certain skin conditions, such as acne, chronic boils, and many cases of eczema.
It may be noted at this point that the most delicate test of the correct application of the two rules given above lies in the disappearance of this offensiveness from the motions, etc.
Applying the Rules
In spite of the simplicity of the diet, it is essential to know the following points about its practical application.
1. Flour
White flour in the kitchen has to be replaced by a true wholemeal flour. The latter flour can be bought or ordered from a good grocer, but it is far from easy to lay your hands on a true wholemeal bread. Many brown breads are by no means wholemeal. This matter will probably need consultation with your baker, or ‘health shop’. There are also books on sale showing how you can bake a true wholemeal bread yourself, without any kneading (the Doris Grant method — Your Daily Food, 1973, London: Faber & Faber).
Next, it is essential not to eat your bread too new. New bread forms pasty lumps in the mouth, which do not properly mix with the saliva and are exceedingly indigestible. Bread should therefore be exposed to the air for at least two days before it is eaten. This should be done by wrapping it up in a cloth, not enclosing it in a tin (which fosters mildew).
In the eating of rice or a refined breakfast cereal, a tablespoonful of unprocessed bran, as described below, could be added to each plateful, to restore what has been removed. This would not be necessary with an unrefined cereal like Shredded Wheat or All-Bran. The former may be rendered crisper by slight toasting in an oven. Sugar must only be used sparingly with all these (see below).
2. Sugar
The chief problem in the present diet, however, concerns how to avoid eating ordinary sugar, and all the sweet things containing it. The ideal solution to this problem, undoubtedly, lies in substituting natural sugar, by eating raw fruit or dried fruit (but not tinned fruit, as this contains added sugar). For example, instead of sweetening a rice pudding with sugar, eat a banana or two with it, or make the pudding with some raisins. The substitution of raw fruit involves little or no loss in pleasure, but it does involve some extra expense.
If sugar is taken at all, it should be taken all the way along a meal. This not only protects the gastric membranes, but also heavily reduces sugar consumption. Many people prefer this method of taking sugar anyway. Far the safest way of doing this is to eat a few raisins intermittently, but other, less safe examples are a little sweetened tea accompanying fish or egg meals; some limejuice in the water with meat meals; or a little red-currant jelly or similar substance taken with mutton or other meat; or a little sweetened apple sauce taken with pork. In all cases this sugary material must be taken sparingly, and sweet courses must be omitted altogether. A marmalade with much peel and little sweetness is permissible but most jams are far too sweet to be safe, unless used in exceedingly small quantities. Fresh fruit, being a natural material, can be taken at any time, but it must not be sweetened with much sugar, even after it has been stewed.
It should be added that although honey appears to be a natural food, it should be taken just as sparingly as ordinary sugar. Under natural conditions mankind would have great difficulty in getting honey away from the bees, and even Solomon advised using it in very small quantities. Similarly, the date, containing some ten times as much sugar as an English apple, is not a natural food for the white races, and should be taken sparingly, preferably with other things, such as a glass of milk, which is a very pleasant combination. Bananas and milk also form a very pleasant combination.
It must also be realized, especially in cases of obesity, that beer and similar drinks contain large quantities of malt sugar, and are immensely fattening.
Finally, the use of the chemical substance, saccharin, is not an obvious solution to the avoidance of sugar-consumption, since it is an unnatural material. For this reason, the suggestions set out above are considered unquestionably preferable.
3. Ready-mixed Foods
Avoid eating these, the reason being as follows: If, to take a simple example, you eat boiled eggs, bread, butter, and even a little sweetened tea, in accordance with your personal tastes, you will consume the quantities of each of these foods you are best able to digest; but if the eggs, flour, butter, and sugar are all mixed up by someone else, like the cook when making a cake, the proportions of each may not be nearly so accurately attuned to your particular digestion. This is also the reason why fried foods are often difficult to digest. For with these, if you are a Jack Sprat, you will be forced to eat fat you do not want, in order to eat eggs, fish, meat, or potato you do want.
4. Cooking
The closer food is to the natural state, and the less it is cooked up, the better. Overcooked brown meat, for example, is less easily chewed and digested than underdone red meat. Boiled and steamed foods are still more easily digested. Pickled foods are even further from the natural state than overcooked foods. The lean parts of ham and bacon have been considerably altered from the natural state and should be approached with caution.
As regards potatoes, it is recommended that these be boiled, and eaten with the skins still left in position. They are not then more fattening than any other natural food. Boiled potatoes are clearly more easily digested than baked, roasted, or fried potatoes.
5. Acid Stimulants
Certain foods strongly stimulate the flow of gastric acid, but neutralize none of it. Such foods include coffee, meat extracts, and especially alcohol. These foods are to be avoided, especially in those who suffer from indigestion and ulcer. They are at their most dangerous when taken by themselves.
6. Sandwiches
These are also likely to cause trouble with anyone who suffers from indigestion, unless carefully planned. First of all the bread must be as described above. Next, the amount of butter must be the amount desired by you. Then, if you do not like bread and butter when eating meat, but do like it when eating cheese, sardines, or eggs, make your sandwiches with one of the latter. Lastly, any unwanted bread in the sandwiches should be left uneaten.
7. Tinned Foods
These are not actually harmful, unless they contain added sugar, as in tinned fruit, but fresh foods are always much more appetizing, and are therefore much to be preferred.
8. The Teeth
It is most difficult to digest raw fruit and other desirable natural foods if they cannot be properly masticated. Therefore, it is quite essential that the bite, if inadequate, should be rectified by proper dental treatment, Until this is completed, natural foods should be mashed up carefully before being eaten.
9. The Use of Bran
The present diet will itself usually correct constipation. If it does not, do not resort to drugs but have resort instead to ordinary unprocessed bran, which can be obtained from corn and seed merchants, health stores, and even pet shops. The cost is quite negligible. The bran should be taken at first in teaspoonful doses before meals (otherwise the stomach may become overfilled), and the dose gradually increased, if necessary, to suit individual needs. For example, some people may need several tablespoonfuls a day. Bran cannot be swallowed in the dry state and is best taken in porridge or soup, or in unrefined breakfast cereals with milk, or just washed down in a glass of water. It is sure to cause some flatulence at first, but this slowly vanishes. (If the bread is made at home, a good thing to do is to incorporate extra bran into the flour — up to 10 per cent by weight of the wholemeal flour — thus making a ‘bran-plus’ loaf.)
10. Changes in Diet to be made gradually
Lastly, and perhaps most important of all, the transition to the present diet must be made slowly, so as at all times to keep in step with the appetite — i.e., with the liking for the natural foods indicated.
Summary and Conclusion
An effort has been made to set out the basis of a natural diet, which may be expressed as ‘follow the natural instinct of appetite, as long as it is allowed to play on natural foods’. Both halves of this statement are essential. Eating natural foods that you do not desire will achieve very little; and eating unnatural foods that you do desire will achieve infinitely less.
Since we have become adapted to cooking over thousands of years, foods showing simple cooking count as natural, but refining by machinery is so recent a practice that we are not adapted to it at all. That is why foods containing white flour and white or brown sugar are exceedingly dangerous. If these two groups of foodstuff are avoided, and with due regard to the few items mentioned above, you can and should eat whatever you like, such as meat, fish, eggs, cheese, milk, butter, and any fruit or vegetable.
It must be noted, however, that though the alterations recommended in the diet are so few, they must be very carefully followed. These notes must be frequently consulted and the correct habits built up and maintained. Success will depend on realizing it is health, above all, that governs happiness, so that first things are put first and kept that way. People are prepared to take endless trouble over the maintenance of a motor car, but over the maintenance of that infinitely more delicate mechanism, the human body, they are seldom prepared to take any trouble at all.
Addition
The ‘Grant’ loaf
This quick and easy no-kneading-needed wholemeal bread recipe was publicised widely by Doris Grant in England during World War II to encourage working women to eat well despite food rationing. The loaf is dark, moist and delicious.
500g wholemeal flour
1/8 tsp salt (adjust to preference)
1 level tsp dried yeast
400 ml warm water (about 40 deg C)
Mix the yeast with the warm water in a bowl and keep warm until frothy (about 10 minutes). Add all the flour and the salt. Mix well. Put the mixture into a greased bread tin and leave in a warm place for about 30 minutes to rise. Don’t leave it too long or it can sink again — if this happens mix again and let it rise a second time. Bake in a very hot oven for 20-30 minutes. When done the bread should come away from the sides of the tin easily. Tip it out onto a wire grid to cool.