Diabetes whilst identified, was rare in those on pre-industrialised diets. (See Donnison table page 11 and 13,14,15 Other sources on western disease on non western-groups ) It appears to be a disease of ‘urbanisation so civilisation’ also called ‘Western Diseases”. Donnison also notes the figures shown, even though low, are likely higher than seen in the general indigenous population, presumably due to access by some to western foods.Whilst there is often focus on carbohydrates and particularly simple sugars in relation to diabetes 2, it arguably has multi-factoral origins, including in addition to carbohydrate related causes, imbalances in lipid and antioxidant pathways, and dysfunction in the energy pathways, which will be outlined part by part below in due course.
Rising diabetes levels
“8.5% of adults worldwide has diabetes” – BBC news” 6th April 2016
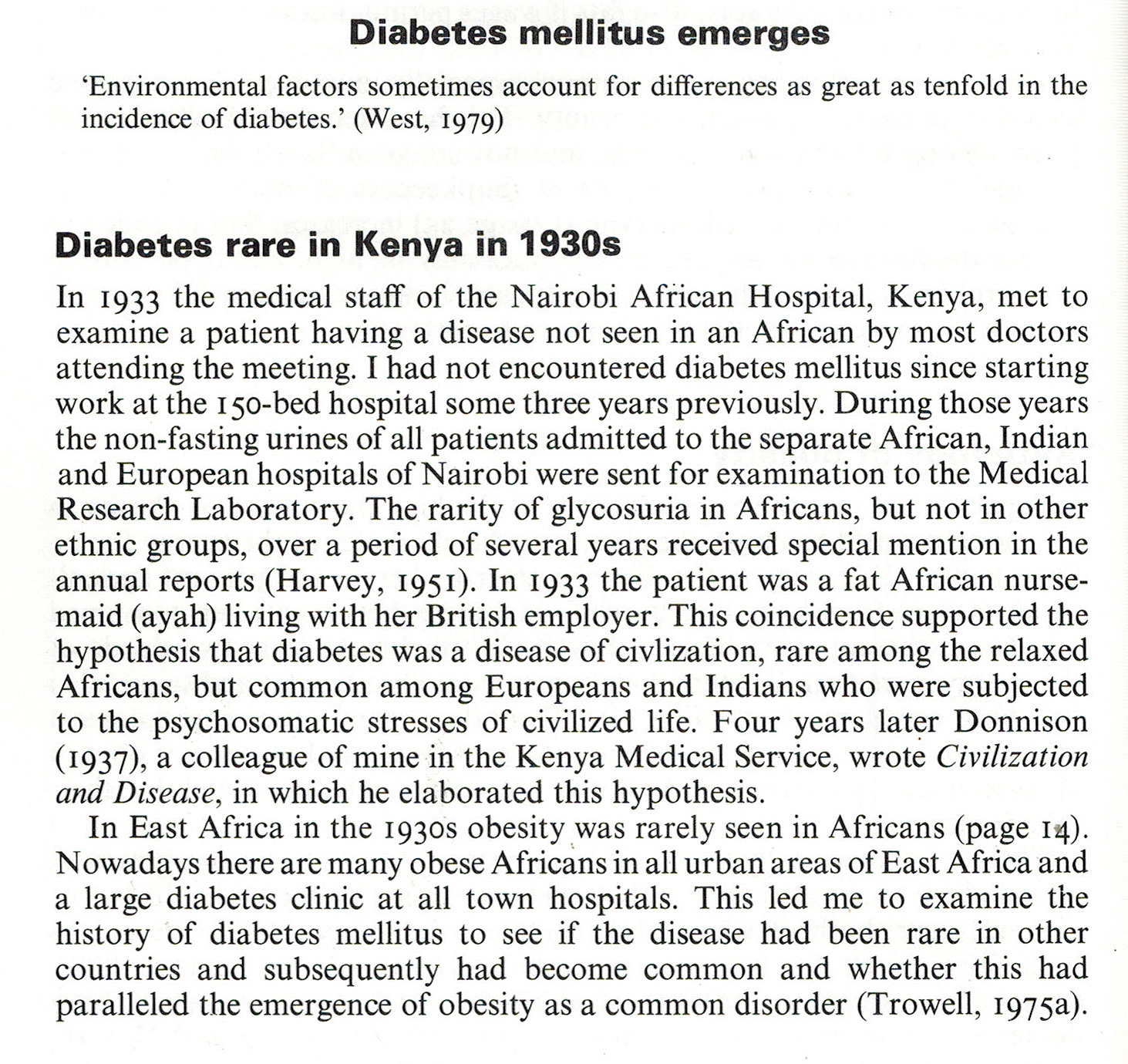
Trowell – In 1933 many Doctors in Kenya had never before seen diabetes in an African
From Western Disease; their emergence and prevention. Burkitt and Trowell Ch1, page 22. Edward Arnold
Cleave and diabetes
Cleave’s book The Saccharine Disease, chapter 7 “On the Causation of Diabetes” is available on line free
(Link) and starts Times New Roman,Georgia,Times; On the Causation of Diabetes
Preliminary Considerations
SOME twenty years ago, that is, in 1955, if the incidence of diabetes was being related to the consumption of any particular class of foodstuff, it was being related to the consumption of fats. This was largely due to a paper by H. Himsworth (1949), [1] who showed that during the 1939-45 war, when the diabetes mortality fell steeply in all the countries that experienced food-rationing, the only class of foodstuff to show a coincident fall in consumption was the fats; the carbohydrates and proteins showed an actual rise. After demonstrating this relationship, Himsworth continued: ‘There is a mass of evidence with similar import. The progressive rise in diabetic mortality in Western countries during the last fifty years coincides with a gradual change towards higher fat and lower carbohydrate diets; the protein and caloric values have altered little… But that is not to say that fat is the deleterious factor; it may simply serve as an indicator of other and more important contingent variables.” (Link)
Thought provoking indeed. (I have almost fortutioulsy found a copy of Himsworth’s paper by after much searching in libraries including the British Library, which paper I will post in due course. Himsworth position was more nuanced, at least in later years than Cleaves then summary suggests – more information available today would suggests there were merits in both arguments in that both particular fats and refined carbohydrates, with other declines in dietary quality arguably factor in development of diabetes.) Arguably fats and particularly Omega 6 linoleic acid and its oxidised products in excess, and in the context of a ‘western’ diet, are co-factors in Diabetes 2, as are refined foods rather than just carbohydrate intake.